

Comparison of Prognosis between Abdominal and Laparoscopic Radical Hysterectomies in Early-stage Cervical Cancer: A Retrospective Cohort Study
- PMID: 40786667
- PMCID: PMC12334104
- DOI: 10.4103/gmit.GMIT-D-24-00033
Comparison of Prognosis between Abdominal and Laparoscopic Radical Hysterectomies in Early-stage Cervical Cancer: A Retrospective Cohort Study
Abstract
Objectives: There is still ongoing debate regarding the surgical approach for early-stage cervical cancer. We aimed to compare the outcomes of abdominal radical hysterectomy (ARH) and laparoscopic radical hysterectomy (LRH) in patients with early-stage cervical cancer and compare our results with those of previous studies.
Materials and methods: This study included patients with early-stage cervical cancer (International Federation of Gynecology and Obstetrics ≤ stage IIA) who received treatment from January 2002 to December 2022. Clinical, surgical, pathological, recurrence, and survival data were collected and analyzed using suitable statistical methods.
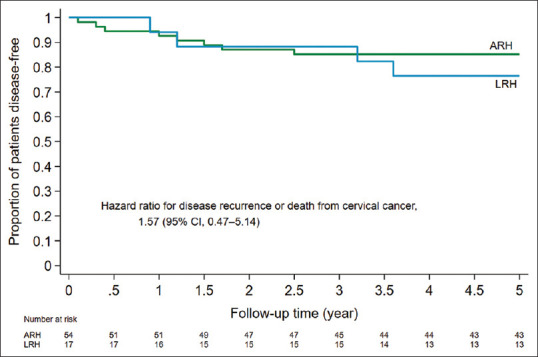
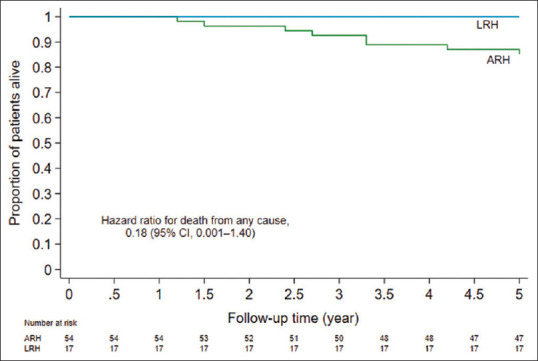
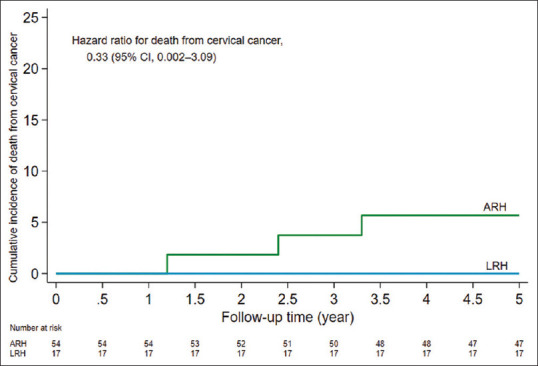
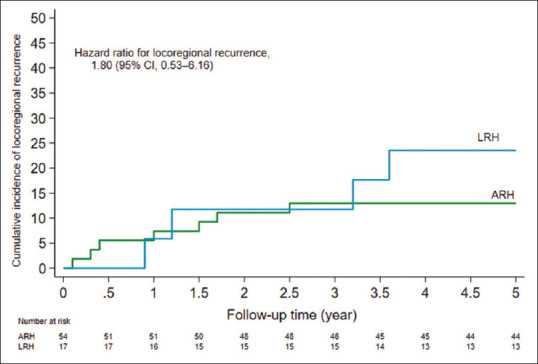
Results: Of the 71 patients, 54 underwent ARH and 17 underwent LRH. The median follow-up durations were 117.0 months for the ARH group and 64.4 months for the LRH group. The average age of patients was 53.7 years, with a mean body mass index of 24.2 kg/m2. Most patients had stage IB1 disease, and squamous cell carcinoma was the most common histological type. ARH was performed in 76.1% of patients, while 23.9% underwent LRH. LRH patients had significantly less blood loss (180 ml vs. 871.7 ml) and shorter hospital stays (6 days vs. 14 days). No significant differences in disease recurrence, cervical cancer-related mortality, or overall survival were observed between the two groups.
Conclusion: Early-stage cervical cancer patients who received LRH had survival and recurrence outcomes comparable to those who underwent ARH.
Keywords: Cervical cancer; minimally invasive surgery; open surgery; recurrence; survival.
Copyright: © 2025 Gynecology and Minimally Invasive Therapy.
Conflict of interest statement
Dr. Dah-Ching Ding, an editorial board member at Gynecology and Minimally Invasive Therapy, had no role in the peer review process of or decision to publish this article. All authors declared no conflicts of interest in writing this paper.
Figures
Similar articles
-
Laparoscopic radical hysterectomy with Karez technique for stage IB3 and IIA2 cervical cancer: a multicenter retrospective cohort study.Int J Surg. 2025 Jul 1;111(7):4516-4527. doi: 10.1097/JS9.0000000000002522. Epub 2025 May 16. Int J Surg. 2025. PMID: 40387736
-
SUCCOR morbidity: complications in minimally invasive versus open radical hysterectomy in early cervical cancer.Int J Gynecol Cancer. 2024 Feb 5;34(2):203-208. doi: 10.1136/ijgc-2023-004657. Int J Gynecol Cancer. 2024. PMID: 38669163
-
Long-Term Oncological Outcomes After Laparoscopic Versus Abdominal Radical Hysterectomy in Stage IA2 to IIA2 Cervical Cancer: A Matched Cohort Study.Int J Gynecol Cancer. 2016 Sep;26(7):1264-73. doi: 10.1097/IGC.0000000000000749. Int J Gynecol Cancer. 2016. PMID: 27643649
-
Hysterectomy with radiotherapy or chemotherapy or both for women with locally advanced cervical cancer.Cochrane Database Syst Rev. 2015 Apr 7;(4):CD010260. doi: 10.1002/14651858.CD010260.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2022 Aug 22;8:CD010260. doi: 10.1002/14651858.CD010260.pub3. PMID: 25847525 Updated.
-
Laparoscopic Radical Hysterectomy in Early Stage Cervical Cancer: A Systematic Review and Meta-Analysis.J Laparoendosc Adv Surg Tech A. 2017 Nov;27(11):1132-1144. doi: 10.1089/lap.2017.0022. Epub 2017 Mar 16. J Laparoendosc Adv Surg Tech A. 2017. PMID: 28300465
References
LinkOut - more resources
Full Text Sources