

Comparative Long-term Outcomes of Laparoscopic Radical Hysterectomy with Sentinel Node Navigation and Open Surgery for Cervical Cancer
- PMID: 40786671
- PMCID: PMC12334094
- DOI: 10.4103/gmit.GMIT-D-24-00003
Comparative Long-term Outcomes of Laparoscopic Radical Hysterectomy with Sentinel Node Navigation and Open Surgery for Cervical Cancer
Abstract
Objectives: Minimally invasive surgery (MIS) for cervical cancer is associated with poorer outcomes compared with open surgery. The Laparoscopic Approach to Cervical Cancer trial revealed an increased recurrence and mortality risk after MIS. We aimed to compare the long-term outcomes of laparoscopic radical hysterectomy (LRH) with those of sentinel node navigation surgery (SNNS) and open surgery for cervical cancer, emphasizing techniques to prevent cancer spillages.
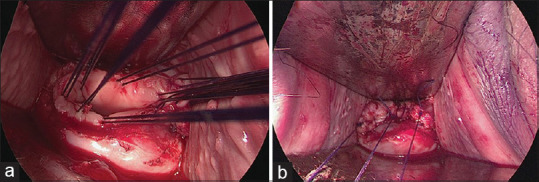
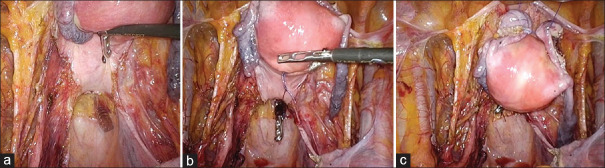
Materials and methods: We retrospectively analyzed data from 103 patients with cervical cancer who underwent radical hysterectomy at Kagoshima University Hospital between 2007 and 2023. The patients were divided into the LRH with SNNS and open surgery groups. All LRH procedures involved closing the vagina using a vaginal cuff without a uterine manipulator. Clinicopathological factors and oncological outcomes, including 5-year recurrence-free survival (RFS) and overall survival (OS), were compared between the groups.
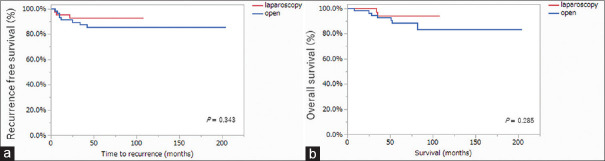
Results: The 5-year RFS and OS rates were 92.7% and 94% and 85.5% and 88.3% for LRH and open surgery, respectively, with no significant intergroup differences. No peritoneal dissemination or recurrence was observed in the LRH group. LRH with SNNS procedure achieved 100% sentinel node identification, and lower extremity lymphedema or pelvic lymphocele did not occur.
Conclusion: LRH with SNNS and open surgery for cervical cancer exhibited comparable long-term outcomes. Vaginal closure using a vaginal cuff without a uterine manipulator is crucial for preventing cancer spillage. Combining LRH with SNNS is less invasive and avoids compromising oncological outcomes. High-quality randomized controlled trials are required to validate these findings.
Keywords: Colpotomy; hysterectomy; lymphedema; minimally invasive surgery; sentinel lymph node.
Copyright: © 2025 Gynecology and Minimally Invasive Therapy.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Hysterectomy with radiotherapy or chemotherapy or both for women with locally advanced cervical cancer.Cochrane Database Syst Rev. 2015 Apr 7;(4):CD010260. doi: 10.1002/14651858.CD010260.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2022 Aug 22;8:CD010260. doi: 10.1002/14651858.CD010260.pub3. PMID: 25847525 Updated.
-
Laparoscopic radical hysterectomy with Karez technique for stage IB3 and IIA2 cervical cancer: a multicenter retrospective cohort study.Int J Surg. 2025 Jul 1;111(7):4516-4527. doi: 10.1097/JS9.0000000000002522. Epub 2025 May 16. Int J Surg. 2025. PMID: 40387736
-
Lymphadenectomy or sentinel node biopsy for the management of endometrial cancer.Cochrane Database Syst Rev. 2025 Jun 10;6(6):CD015786. doi: 10.1002/14651858.CD015786.pub2. Cochrane Database Syst Rev. 2025. PMID: 40492478 Review.
-
Comparative Outcomes of Laparoscopic Radical Hysterectomy and Nerve-Sparing Technique in Cervical Cancer Patients.JSLS. 2025 Apr-Jun;29(2):e2024.00073. doi: 10.4293/JSLS.2024.00073. Epub 2025 May 13. JSLS. 2025. PMID: 40365089 Free PMC article.
-
Minimally invasive surgical techniques versus open myomectomy for uterine fibroids.Cochrane Database Syst Rev. 2014 Oct 21;2014(10):CD004638. doi: 10.1002/14651858.CD004638.pub3. Cochrane Database Syst Rev. 2014. PMID: 25331441 Free PMC article.
References
-
- Bansal N, Herzog TJ, Shaw RE, Burke WM, Deutsch I, Wright JD. Primary therapy for early-stage cervical cancer: Radical hysterectomy versus radiation. Am J Obstet Gynecol. 2009;201:485.e1–9. - PubMed
-
- Koh WJ, Abu-Rustum NR, Bean S, Bradley K, Campos SM, Cho KR, et al. Cervical cancer, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17:64–84. - PubMed
-
- Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997;350:535–40. - PubMed
-
- Ditto A, Martinelli F, Mattana F, Reato C, Solima E, Carcangiu M, et al. Class III nerve-sparing radical hysterectomy versus standard class III radical hysterectomy: An observational study. Ann Surg Oncol. 2011;18:3469–78. - PubMed
LinkOut - more resources
Full Text Sources