

Vulvar Pressure Ulcer - An Inadvertent Complication of Thomas Splint: Case Report
- PMID: 40786803
- PMCID: PMC12328941
- DOI: 10.13107/jocr.2025.v15.i08.5916
Vulvar Pressure Ulcer - An Inadvertent Complication of Thomas Splint: Case Report
Abstract
Introduction: Pressure ulcers are common complications in immobilized patients, typically occurring over bony prominences. However, in rare instances, particularly in high-risk individuals with hematologic disorders such as sickle cell disease, ulcers may develop at unusual anatomical sites due to external medical devices. This case highlights a rare presentation of a vulvar pressure ulcer caused by prolonged application of a Thomas splint in a patient with homozygous sickle cell disease (HbSS).
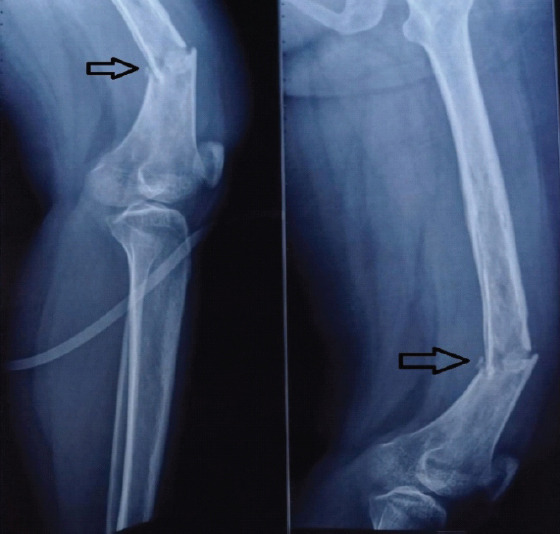
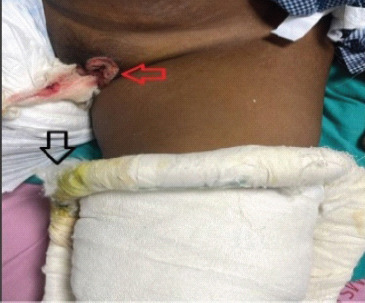
Case report: A 24-year-old woman with HbSS was admitted with a closed distal femoral shaft fracture. She was immobilized using a Thomas splint. On the 15th day of hospitalization, she developed a necrotic ulcer over the labia majora, diagnosed as a vulvar pressure ulcer secondary to device compression. Conservative wound management was initiated, followed by surgical debridement and closure using local advancement flaps. Orthopedic care was modified, and internal fixation of the fracture was later performed in a pressure-avoiding position. The wound healed completely within 2 weeks of surgery.
Conclusion: Vulvar pressure ulcers are rare and often underdiagnosed, particularly in patients with risk factors like sickle cell disease. This case emphasizes the need for regular inspection of pressure points, patient education, and multidisciplinary collaboration to prevent and manage such complications. Thoughtful application and monitoring of immobilization devices can reduce the risk of pressure injuries in vulnerable populations.
Keywords: Pressure ulcer; Thomas splint; orthopedic complication; sickle cell disease; vulvar wound.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures





References
-
- Bergstrom N, Horn SD, Smout RJ, Bender SA, Ferguson ML, Taler G, et al. The national pressure ulcer long-term care study:Outcomes of pressure ulcer treatments in long-term care. J Am Geriatr Soc. 2005;53:1721–9. - PubMed
-
- Mancoll JS, Phillips LG. Pressure sores. In: Achauer BM, Erikson E, Guzuron B, Coleman J 3rd, Russell R, Vander Kolk C, editors. Plastic Surgery. Vol. 1. St. Louis, MO: Mosby Inc; 2000. pp. 447–62.
-
- Conde Montero E, Martínez Gómiz JM, De La Cueva Dobao P. The vulva:An uncommon presentation of a pressure ulcer. Wounds. 2017;29:E28–31. - PubMed
-
- Rathore FA, New PW, Waheed A. Pressure ulcers in spinal cord injury:An unusual site and etiology. Am J Phys Med Rehabil. 2009;88:587–90. - PubMed
Publication types
LinkOut - more resources
Full Text Sources