

Challenges in Diagnosing Diaphyseal Osteosarcoma - Importance of Strong Clinical Suspicion and Biopsy Technique: An Illustrative Case Report
- PMID: 40786805
- PMCID: PMC12328954
- DOI: 10.13107/jocr.2025.v15.i08.5934
Challenges in Diagnosing Diaphyseal Osteosarcoma - Importance of Strong Clinical Suspicion and Biopsy Technique: An Illustrative Case Report
Abstract
Introduction: Osteosarcoma is the most common primary malignant bone tumor in adolescents, typically affecting the metaphyseal region of long bones. Diaphyseal osteosarcoma is rare and often mimics benign conditions such as osteomyelitis, leading to diagnostic delays.
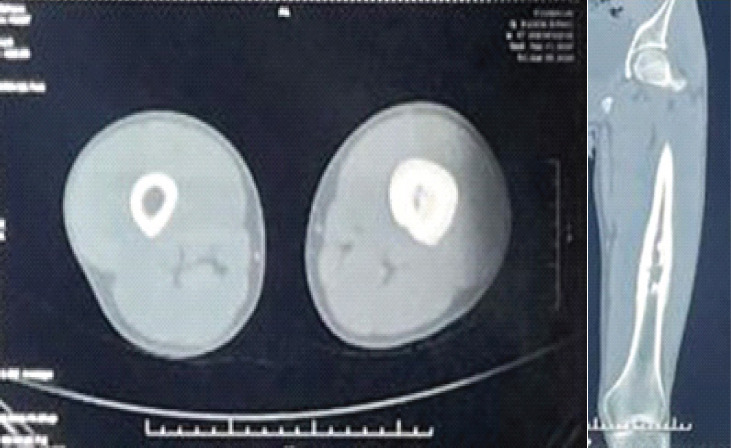
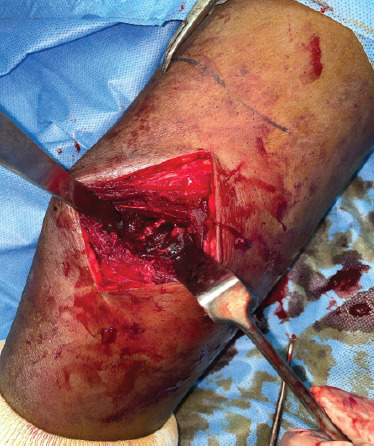
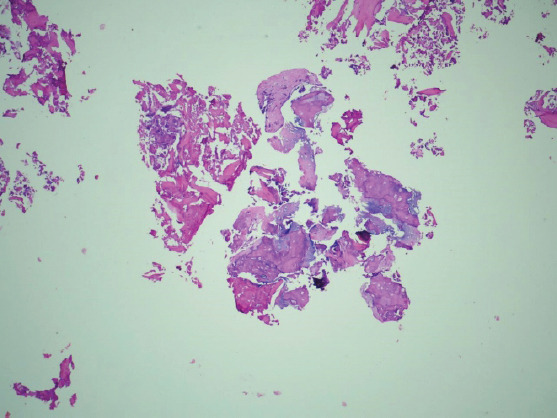
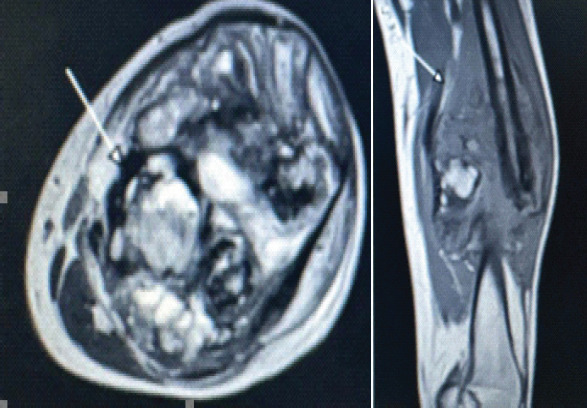
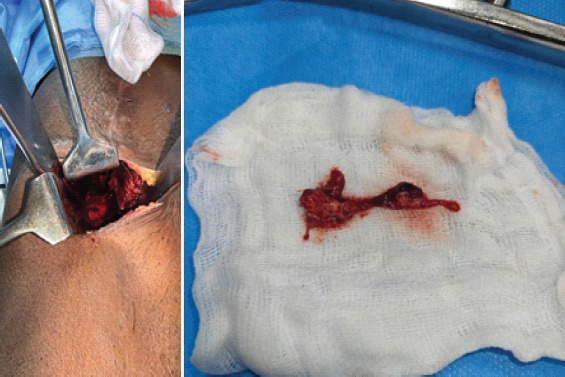
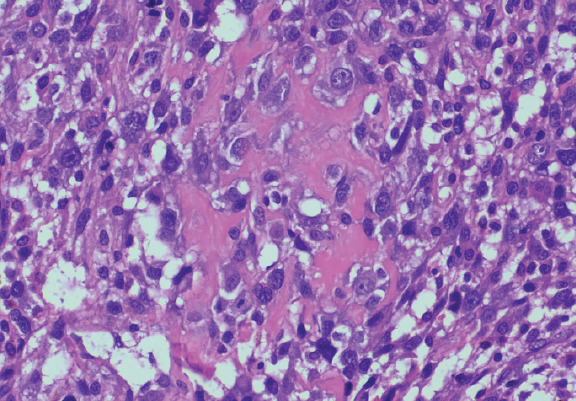
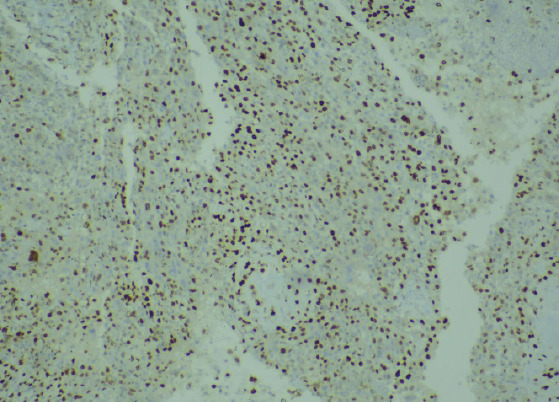
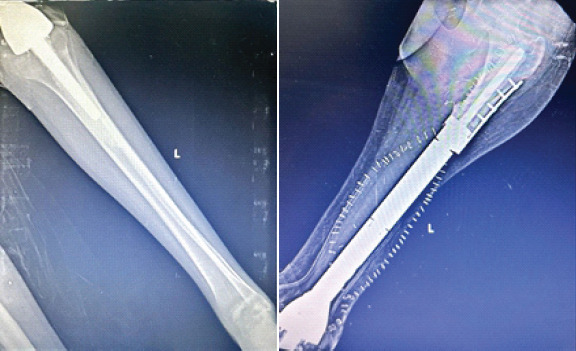
Case report: A 17-year-old boy presented with progressive left thigh pain and swelling for 3 months. He had a trivial injury to left thigh 7 months back while playing kabaddi. Initial radiographs, computed tomography (CT), and magnetic resonance imaging showed a lytic intramedullary lesion with cortical thickening, suggestive of osteomyelitis. CT-guided biopsy also revealed features consistent with chronic osteomyelitis. Later debridement with open biopsy confirmed increased reactive osteoclastic giant cells, suggestive of chronic healed osteomyelitis. Despite empirical antibiotic treatment, symptoms worsened. A second open biopsy with intraoperative frozen section (FS) revealed features of high-grade osteosarcoma. Histopathological confirmation and immunohistochemistry with SATB2 established the diagnosis. The patient was treated with neoadjuvant chemotherapy followed by resection and femur reconstruction with a custom prosthesis.
Discussion: This case illustrates the diagnostic pitfalls associated with diaphyseal osteosarcoma, especially in post-traumatic settings. It has also been observed in previous research studies that early overlapping clinical and radiological features with osteomyelitis often result in misdiagnosis. Needle biopsies, while minimally invasive, may yield non-representative samples, especially in heterogeneous tumors. Open biopsy targeting the lesion's transition zone, supported by intraoperative FS, enhances diagnostic accuracy and enables timely intervention.
Conclusion: In atypical presentations of musculoskeletal pain and swelling unresponsive to conservative treatment, malignancy should be suspected. A multidisciplinary approach, early advanced imaging, and appropriately planned biopsies are critical for accurate diagnosis and effective management of osteosarcoma.
Keywords: Osteosarcoma; computed tomography-guided biopsy; frozen section; open biopsy; osteomyelitis.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures




Similar articles
-
Chronic Nonbacterial Osteomyelitis in a Young Child: A Case Report of a Diagnostic Challenge Mimicking Malignancy.Cureus. 2025 Jun 10;17(6):e85684. doi: 10.7759/cureus.85684. eCollection 2025 Jun. Cureus. 2025. PMID: 40642690 Free PMC article.
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
A Case Report of Acute on Chronic Osteomyelitis of Distal Femur Managed with Sequestrectomy, Saucerization, and Stimulan Placement.J Orthop Case Rep. 2025 Jul;15(7):163-167. doi: 10.13107/jocr.2025.v15.i07.5808. J Orthop Case Rep. 2025. PMID: 40635932 Free PMC article.
-
COL1A1- and COL1A2-Related Osteogenesis Imperfecta.2005 Jan 28 [updated 2025 May 29]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2005 Jan 28 [updated 2025 May 29]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301472 Free Books & Documents. Review.
References
Publication types
LinkOut - more resources
Full Text Sources