

Anatomical Pelvic Parameters Using the Anterior Pelvic Plane: Relationships with Standing Sagittal Spinal Alignment and Estimated Lumbar Alignment in Healthy Volunteers
- PMID: 40786923
- PMCID: PMC12330368
- DOI: 10.22603/ssrr.2024-0283
Anatomical Pelvic Parameters Using the Anterior Pelvic Plane: Relationships with Standing Sagittal Spinal Alignment and Estimated Lumbar Alignment in Healthy Volunteers
Abstract
Introduction: To estimate natural standing sagittal alignment in patients with adult spinal deformity (ASD), we previously reported the normative values of anatomical pelvic parameters in a healthy population, based on the anterior pelvic plane (APP), and observed the relationships between anatomical and positional pelvic parameters in the standing position. As the second step, we aim to investigate the relationships between anatomical pelvic parameters and standing spinal sagittal alignment in a healthy population.
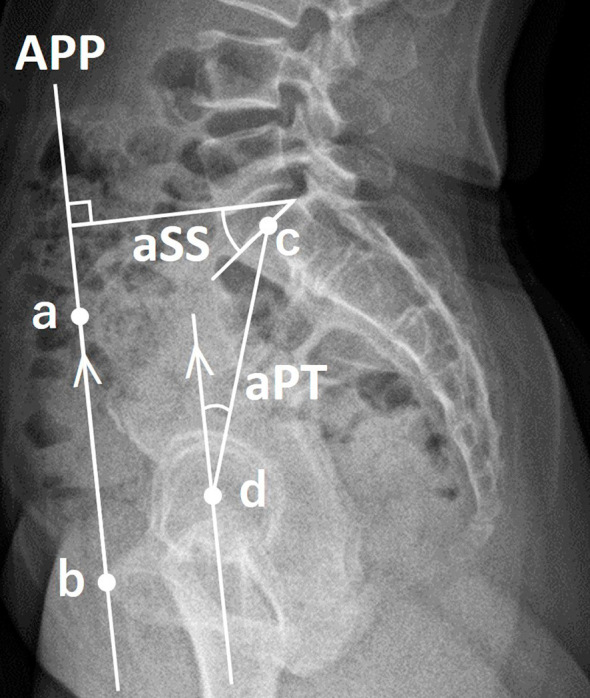
Methods: We analyzed biplanar, slot-scanning, full-body stereo radiography of 140 healthy Japanese volunteers (mean age, 39.5 years; 59.3% women). The APP was defined by bilateral anterior superior iliac spines and anterior surface of the pubis symphysis. Anatomical sacral slope (aSS) and anatomical pelvic tilt (aPT) were calculated as angles of the SS and PT regarding the APP.
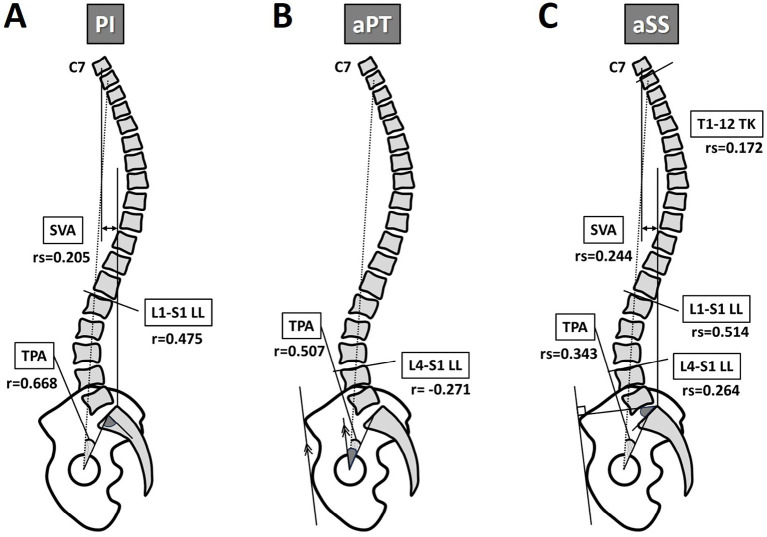
Results: The APP was tilted anteriorly in the sagittal plane by an average of 0.7°. Anatomical pelvic parameters significantly correlated with standing sagittal parameters, except for cervical lordosis and T4-12 thoracic kyphosis (TK) (p<0.05). L4-S1 lumbar lordosis (LL) significantly correlated with aPT and aSS, but not with pelvic incidence (PI). In addition, T1-12 TK significantly correlated with aSS. Multiple linear regression analysis for lumbar alignment produced the following equations: L1-S1 LL (°)=0.588×aSS+30.522, L4-S1 LL (°)=0.165×aSS-0.248×aPT+32.825, lordosis distribution index (%)=-0.662×PI+102.8.
Conclusions: Novel relationships in a healthy population were identified between the anatomical characteristics of the pelvis and standing sagittal parameters not represented by PI. This novel measurement concept based on the APP may estimate natural standing sagittal alignments and proportions using anatomical pelvic parameters in ASD.
Keywords: anatomical pelvic parameter; anterior pelvic plane; lumbar lordosis; lumbar proportion; standing sagittal alignment.
Copyright © 2025 The Japanese Society for Spine Surgery and Related Research.
Conflict of interest statement
Conflicts of Interest: The authors declare that there are no relevant conflicts of interest.
Figures
Similar articles
-
Does Periacetabular Osteotomy Change Sagittal Spinopelvic Alignment?Clin Orthop Relat Res. 2024 Sep 1;482(9):1659-1667. doi: 10.1097/CORR.0000000000003031. Epub 2024 Apr 2. Clin Orthop Relat Res. 2024. PMID: 38564796
-
Anatomical Pelvic Parameters Using the Anterior Pelvic Plane: Normative Values and Estimation of the Standing Sagittal Alignment in Healthy Volunteers.Spine Surg Relat Res. 2023 Nov 2;8(1):97-105. doi: 10.22603/ssrr.2023-0181. eCollection 2024 Jan 27. Spine Surg Relat Res. 2023. PMID: 38343408 Free PMC article.
-
The effect of degenerative scolioisis on segmental thoracolumbar sagittal alignment compared to age- and pelvic incidence-matched reference values.Eur Spine J. 2025 Feb;34(2):764-772. doi: 10.1007/s00586-024-08618-7. Epub 2025 Jan 13. Eur Spine J. 2025. PMID: 39800820
-
Normative Thoracic, Lumbar, Pelvic, and Global Sagittal Alignment Parameters for Asymptomatic Adults: A Systematic Review and Meta-Analysis of >35,900 Volunteers.Spine (Phila Pa 1976). 2025 Sep 1;50(17):1188-1200. doi: 10.1097/BRS.0000000000005274. Epub 2025 May 23. Spine (Phila Pa 1976). 2025. PMID: 40407040 Review.
-
The influence of osteoporotic vertebral fractures on global sagittal alignment in elderly patients: a systematic review and meta-analysis.Eur Spine J. 2023 Jul;32(7):2580-2587. doi: 10.1007/s00586-023-07780-8. Epub 2023 May 24. Eur Spine J. 2023. PMID: 37222801
References
-
- Lafage V, Schwab F, Patel A, et al. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine. 2009;34(17):E599-606. - PubMed
-
- Schwab FJ, Blondel B, Bess S, et al. Radiographical spinopelvic parameters and disability in the setting of adult spinal deformity: a prospective multicenter analysis. Spine. 2013;38(13):E803-12. - PubMed
-
- Diebo BG, Ferrero E, Lafage R, et al. Recruitment of compensatory mechanisms in sagittal spinal malalignment is age and regional deformity dependent: a full-standing axis analysis of key radiographical parameters. Spine. 2015;40(9):642-9. - PubMed
-
- Hasegawa K, Okamoto M, Hatsushikano S, et al. Normative values of spino-pelvic sagittal alignment, balance, age, and health-related quality of life in a cohort of healthy adult subjects. Eur Spine J. 2016;25(11):3675-86. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous