

Clinical and Imaging Characteristics of Patients with Cervical Compressive Myelopathy Presenting with Unilateral Motor Deficits
- PMID: 40786928
- PMCID: PMC12330374
- DOI: 10.22603/ssrr.2024-0264
Clinical and Imaging Characteristics of Patients with Cervical Compressive Myelopathy Presenting with Unilateral Motor Deficits
Abstract
Introduction: Cervical compressive myelopathy is a leading cause of spinal cord dysfunction in middle-aged and older adults. Although the pathological classification of cervical myelopathy is well established, the quantitative analysis of its imaging features remains underexplored. This study quantitatively evaluated the imaging characteristics of unilateral motor deficit cervical compressive myelopathy.
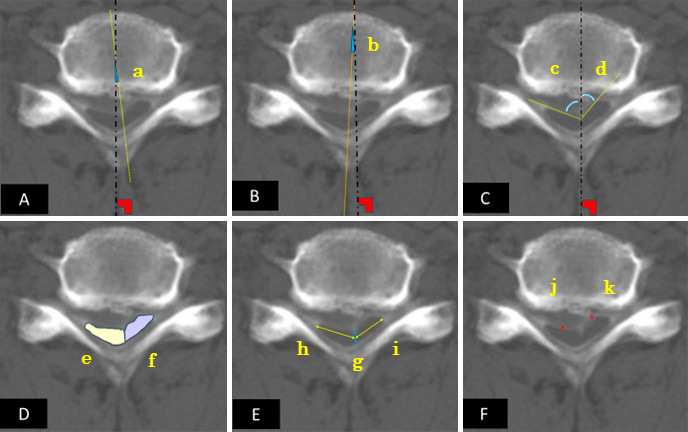
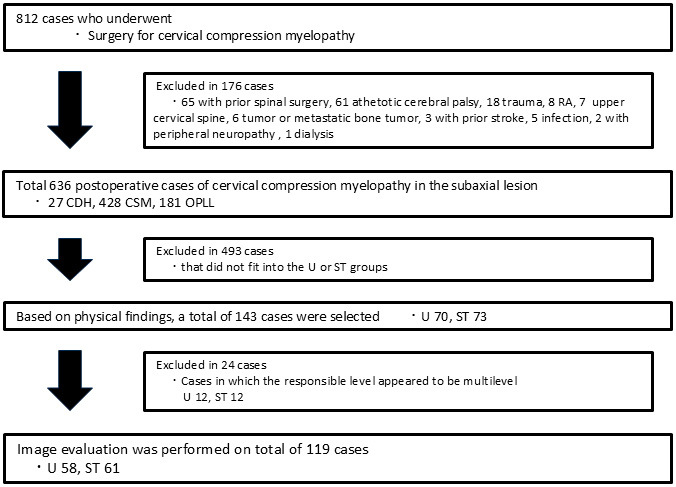
Methods: This retrospective observational study included patients who underwent surgery for cervical compressive myelopathy between 2009 and 2023. Pre-operative cervical magnetic resonance imaging (MRI) and postmyelographic computed tomography (CTM) axial images were assessed for spinal cord rotation, deformity, available space, and signal changes. Patients were classified into unilateral motor deficit (Group U) and symmetric transverse (Group ST) types, and were analyzed for specific imaging parameters.
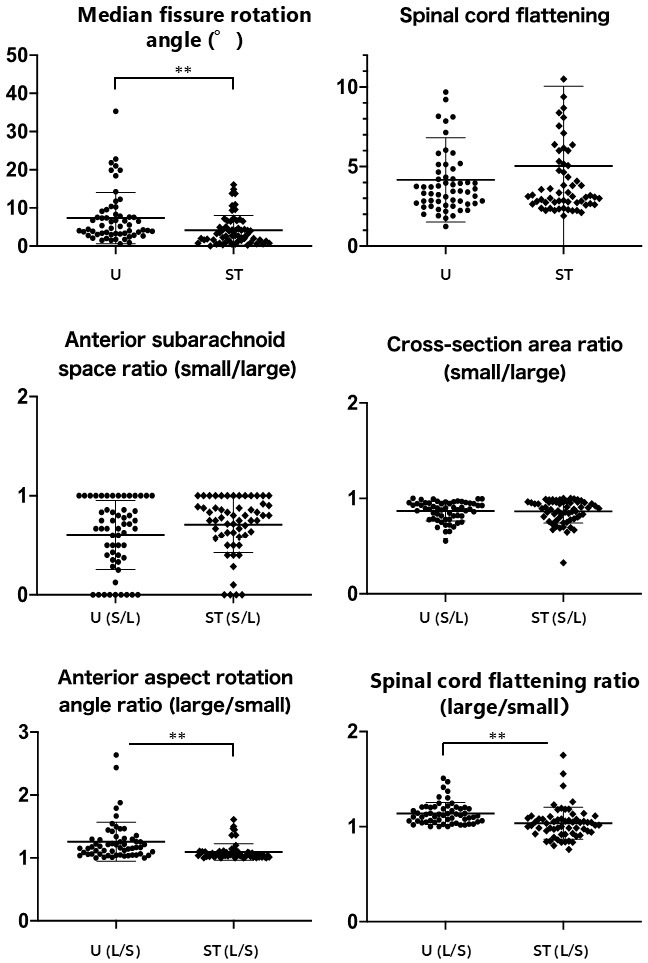
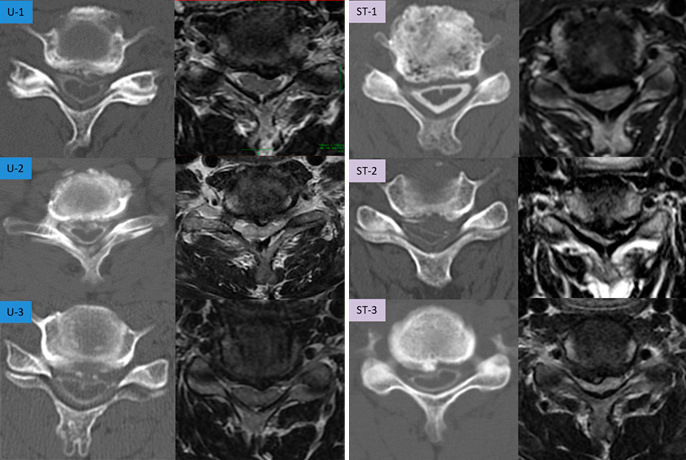
Results: The final analysis included 119 of the 812 identified patients. Group U patients were younger (59.1±13.8 years) and had higher Japanese Orthopaedic Association scores (10.6±2.7) compared with Group ST patients (71.1±11.0 years, 8.4±2.3). Group U showed significant morphological differences, including a reduced anterior-subarachnoid space and increased spinal cord rotation on the affected side. Group U exhibited significant differences in the median fissure rotation angle (7.4°±6.7°) and anterior-aspect rotation angle ratio (1.26±0.31) compared with Group ST (4.14°±3.87°, 1.10±0.14). Receiver operating characteristic curve analysis identified specific cutoff values for distinguishing Group U (2.80° for median fissure rotation angle and 1.116 for anterior-aspect rotation angle ratio). The MRI-based detection sensitivity was lower in Group U (27.6%) compared with in Group ST (68.9%).
Conclusions: Unilateral motor deficits are associated with distinctive spinal cord rotational deformities, including a greater median fissure rotation angle and anterior-aspect rotation angle ratio. CTM is better than MRI for detecting unilateral motor deficits. Future research to improve treatment outcomes should focus on spinal cord circulation assessment using advanced imaging techniques.
Keywords: cerebrospinal fluid space; cervical myelopathy; quantitative imaging analysis; spinal cord rotation; unilateral motor deficit.
Copyright © 2025 The Japanese Society for Spine Surgery and Related Research.
Conflict of interest statement
Conflicts of Interest: The authors declare that there are no relevant conflicts of interest.
Figures

References
-
- Nurjck S. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain. 1972;95(1):87-100. - PubMed
-
- Vijay Kumar GR, Ray DK, Das RK. Natural history, prevalence, and pathophysiology of cervical spondylotic myelopathy. Indian Spine J. 2019;2(1):5-12.
-
- Breig A, Turnbull I, Hassler O. Effects of mechanical stresses on the spinal cord in cervical spondylosis. A study on fresh cadaver material. J Neurosurg. 1966;25(1):45-56. - PubMed
-
- White AA 3rd, Panjabi MM. Biomechanical considerations in the surgical management of cervical spondylotic myelopathy. Spine (Phila Pa 1976). 1988;13(7):856-60. - PubMed
LinkOut - more resources
Full Text Sources