

A Multi-Algorithm Machine Learning Model for Predicting the Risk of Preterm Birth in Patients with Early-Onset Preeclampsia
- PMID: 40786956
- PMCID: PMC12333876
- DOI: 10.2147/IJGM.S521763
A Multi-Algorithm Machine Learning Model for Predicting the Risk of Preterm Birth in Patients with Early-Onset Preeclampsia
Abstract
Purpose: To analyze the risk factors for preterm birth in patients with early-onset preeclampsia (EOPE) based on multi-algorithm machine learning and to construct a predictive model to explore the predictive value of the model.
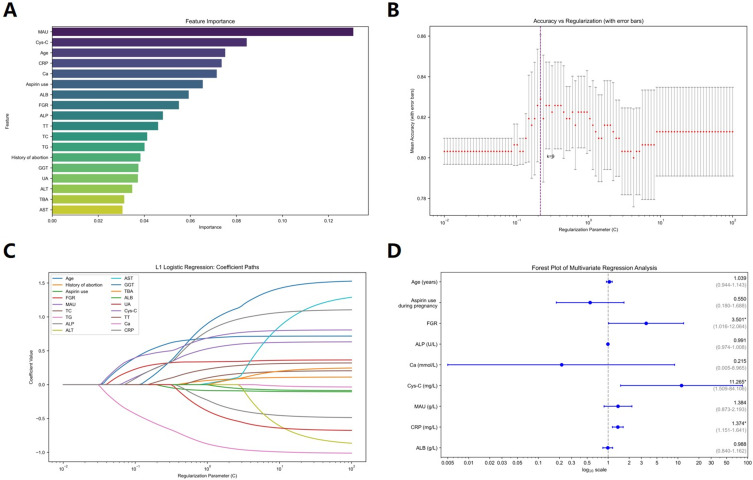
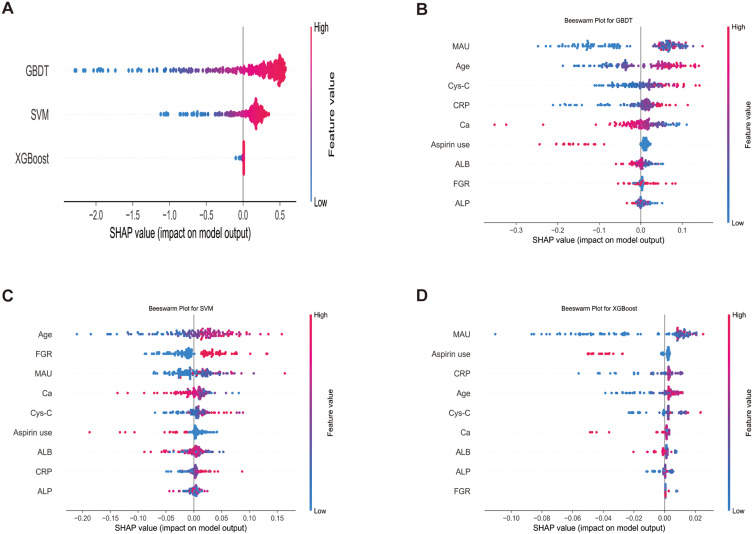
Methods: A retrospective analysis was conducted on 442 EOPE patients from a single tertiary center, divided into preterm birth (<37 weeks, n=358) and term-born (≥37 weeks, n=84) groups. Univariate analysis, random forest importance assessment, lasso regression combined with multivariate regression analysis were used for feature evaluation. Eight machine learning models were trained (70% data) and validated (30% data). A Stacking ensemble model was constructed, and SHapley Additive exPlanations (SHAP) was used for feature interpretation.
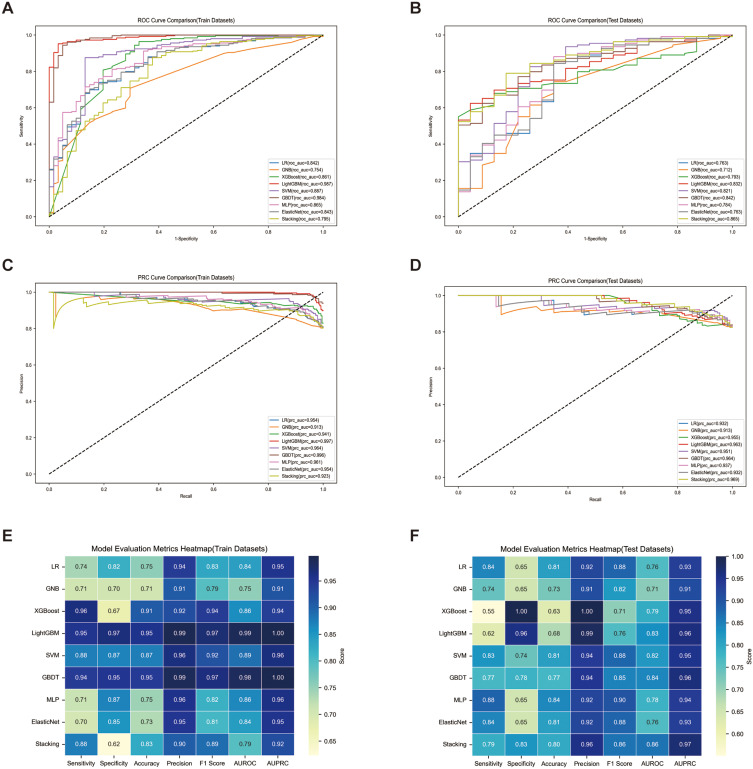
Results: The area under the receiver operating characteristic curve (AUROC) for predicting preterm birth in EOPE patients using Logistic Regression, Gaussian Naive Bayes, Extreme Gradient Boosting (XGBoost), Light Gradient Boosting Machine, Support Vector Machine (SVM), Gradient Boosting Decision Tree (GBDT), Multi-Layer Perceptron, and Elastic Net were 0.763, 0.712, 0.821, 0.832, 0.821, 0.842, 0.784, and 0.763, respectively. The Stacking model (XGBoost+GBDT+SVM) achieved superior performance (AUROC=0.865). Three independent risk factors were identified: fetal growth restriction (aOR=3.50, p = 0.047), serum cystatin C (aOR=11.27, p = 0.018), and C-reactive protein (aOR=1.37, p < 0.001). SHAP analysis revealed GBDT as the top contributor to Stacking predictions, with microalbunminuria (GBDT, XGBoost) and age (SVM) being the most influential features.
Conclusion: Machine learning models can serve as reliable assessment tools for predicting the risk of preterm birth in patients with EOPE. The ensemble prediction model demonstrates the best predictive performance, helping obstetricians identify high-risk patients and perform early intervention to improve perinatal outcomes.
Keywords: clinical prediction model; early-onset preeclampsia; machine learning; preterm birth.
© 2025 Xu et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest in this work.
Figures
Similar articles
-
Supervised Machine Learning Models for Predicting Sepsis-Associated Liver Injury in Patients With Sepsis: Development and Validation Study Based on a Multicenter Cohort Study.J Med Internet Res. 2025 May 26;27:e66733. doi: 10.2196/66733. J Med Internet Res. 2025. PMID: 40418571 Free PMC article.
-
Construction and validation of HBV-ACLF bacterial infection diagnosis model based on machine learning.BMC Infect Dis. 2025 Jul 1;25(1):847. doi: 10.1186/s12879-025-11199-5. BMC Infect Dis. 2025. PMID: 40596896 Free PMC article.
-
Differential Predictability of Preterm Birth Types: Strong Signals for Indicated Cases versus Limited Success in Spontaneous Preterm Birth.medRxiv [Preprint]. 2025 Jul 10:2025.07.09.25329712. doi: 10.1101/2025.07.09.25329712. medRxiv. 2025. PMID: 40672516 Free PMC article. Preprint.
-
Interpretable machine learning for predicting isolated basal septal hypertrophy.PLoS One. 2025 Jun 30;20(6):e0325992. doi: 10.1371/journal.pone.0325992. eCollection 2025. PLoS One. 2025. PMID: 40587445 Free PMC article.
-
Predicting the risk of lean non-alcoholic fatty liver disease based on interpretable machine models in a Chinese T2DM population.Front Endocrinol (Lausanne). 2025 Jul 11;16:1626203. doi: 10.3389/fendo.2025.1626203. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40717804 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials
