

Youth Uptake of Digital Sexual and Reproductive Health Services Across Sociodemographic Groups (2018-2022): A Total Population Study from Stockholm, Sweden
- PMID: 40787430
- PMCID: PMC12332933
- DOI: 10.1016/j.mcpdig.2025.100251
Youth Uptake of Digital Sexual and Reproductive Health Services Across Sociodemographic Groups (2018-2022): A Total Population Study from Stockholm, Sweden
Abstract
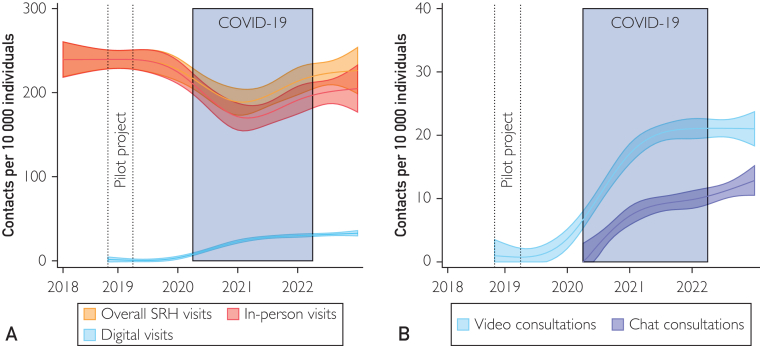
Objective: To examine uptake of in-person and digital sexual and reproductive health (SRH) services among adolescents and young adults, quantify uptake across time, and explore whether the introduction of digital services affected the sociodemographic composition of users.
Patients and methods: This Swedish total population study included all Stockholm residents aged 12-22 years between January 1st 2018 and December 31st 2022. The primary outcome was in-person or digital visits (chat and video) of SRH services within a year, identified using regional health care registries. Sociodemographic predictors included sex, age, migrant background, parental education, and household income, analyzed with repeated-measures multivariable regressions.
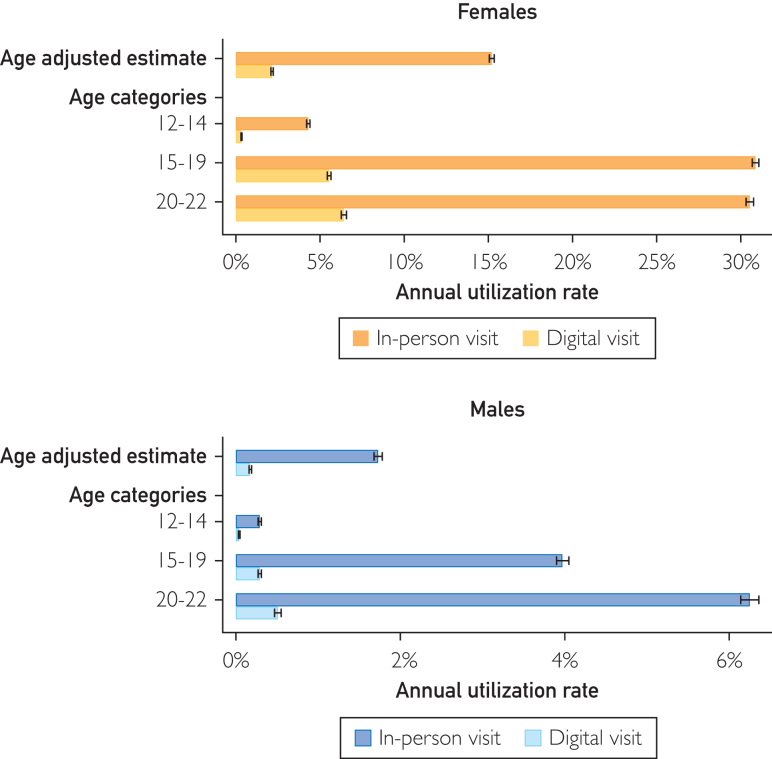
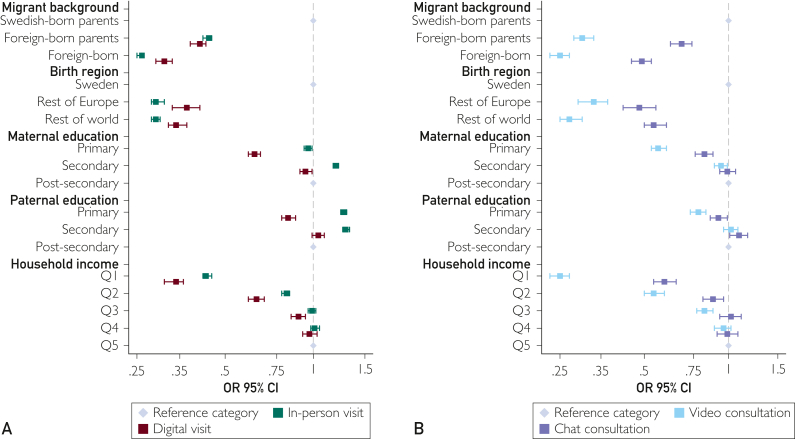
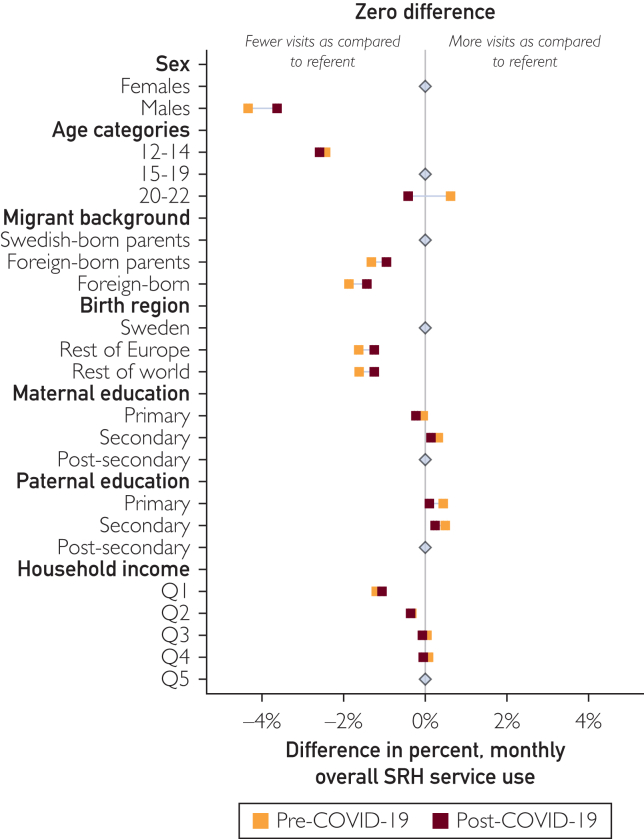
Results: Among the 454,405 individuals, 23.96% had at some point used SRH services (80.01% women) between 2018 and 2022. In-person visits remained the predominant mode of contact. Women had higher annual utilization rate of both in-person (women: 15.27%; 95% CI, 15.13-15.40; men: 1.75%; 95% CI, 1.72-1.78) and digital visits (women: 2.23%; 95% CI, 2.16-2.30; men: 0.12%; 95% CI, 0.11-0.13). Significantly lower uptake was also observed in the lowest income quintile (digital: adjusted odds ratio [aOR], 0.34; 95% CI, 0.31-0.36; in-person: aOR, 0.43; 95% CI, 0.42-0.45) compared with the highest quintile (reference group). Among digital visits, chat was more equitably used than video consultations across sociodemographic groups, including smaller differences between the highest and lowest income quintiles (chat: aOR, 0.59; 95% CI, 0.54-0.65; video: aOR, 0.25; 95% CI, 0.23-0.27). Only modest reductions in socioeconomic disparities were observed after the introduction of digital services.
Conclusions: Sociodemographic disparities in utilization were not alleviated by the introduction of digital visits; in-person users were also the primary digital users. Chat could be more equitable than video, but further research is needed.
© 2025 The Authors.
Conflict of interest statement
The authors report no competing interests.
Figures
References
-
- World Health Organization . World Health Organization; 2022. Consolidated Telemedicine Implementation Guide.
-
- Lawrence K. In: Digital Health. Linwood S.L., editor. Exon Publications; 2022. Digital health equity; pp. 121–130. - PubMed
LinkOut - more resources
Full Text Sources
