

Hysteroscopic Myomectomy for Type 2 Submucosal Myoma Pretreated by HIFU and Mifepristone Treatment: A Case Report and Literature Review
- PMID: 40787589
- PMCID: PMC12333630
- DOI: 10.2147/IJWH.S530879
Hysteroscopic Myomectomy for Type 2 Submucosal Myoma Pretreated by HIFU and Mifepristone Treatment: A Case Report and Literature Review
Abstract
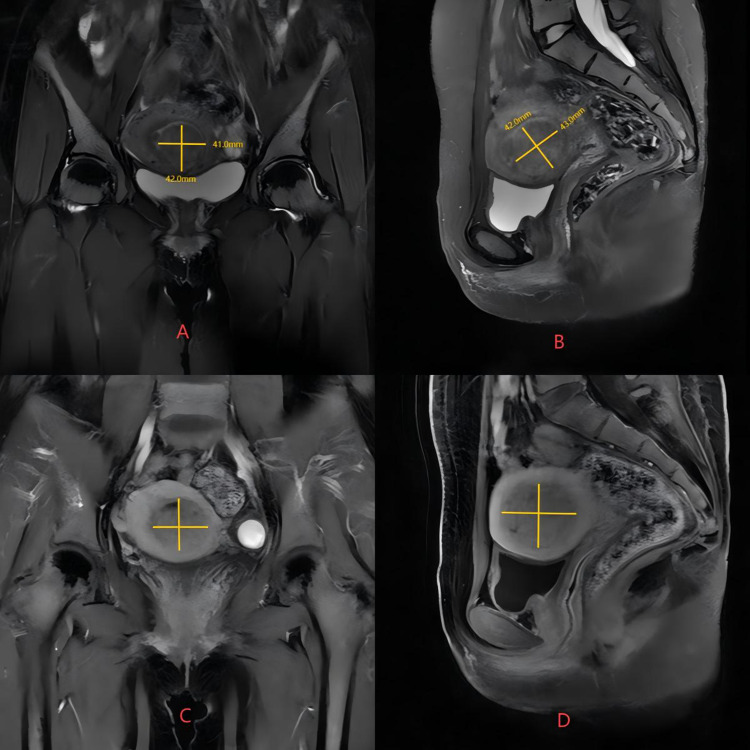
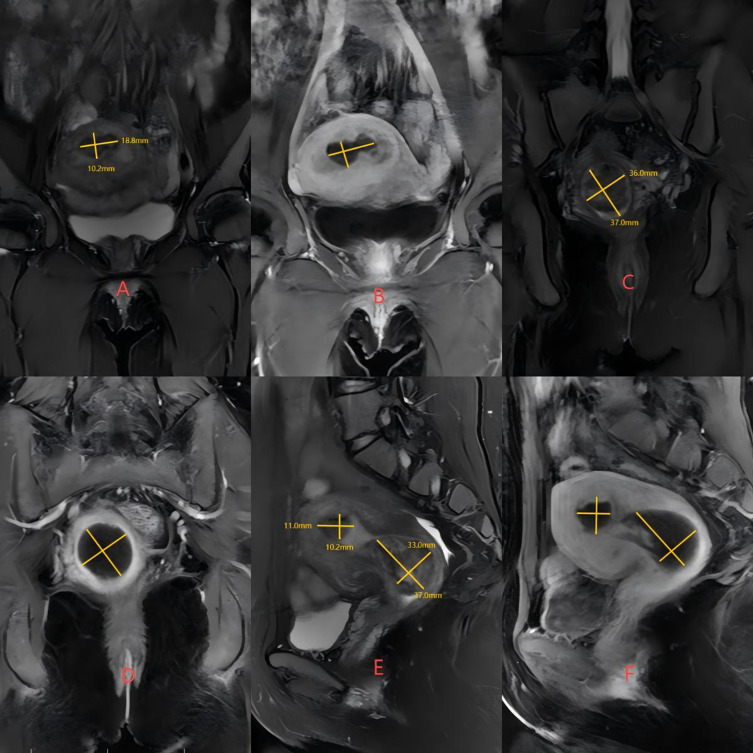
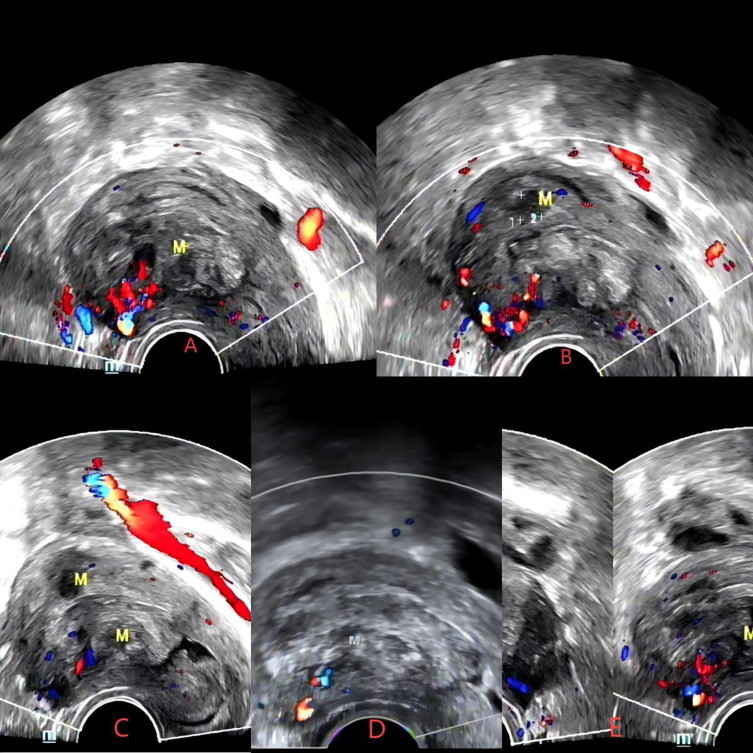
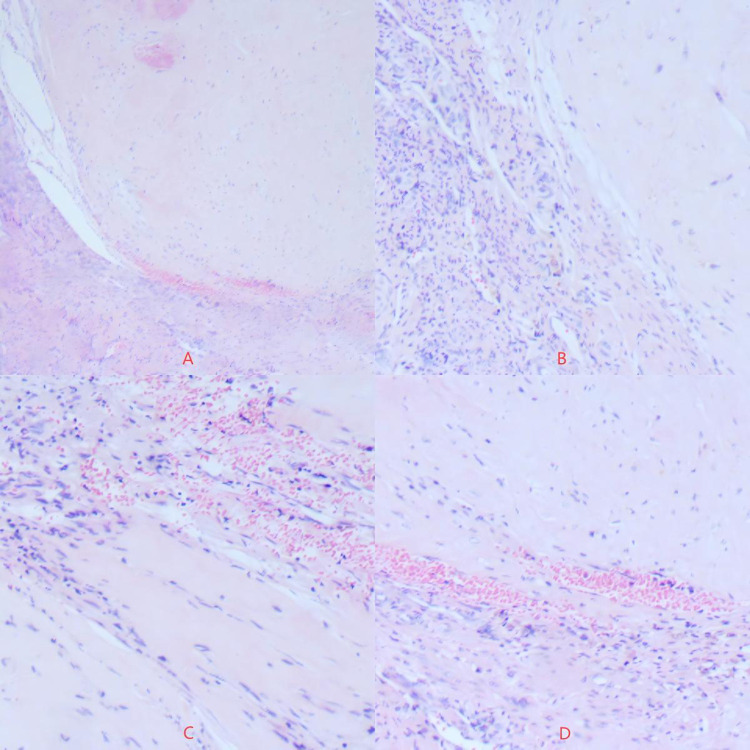
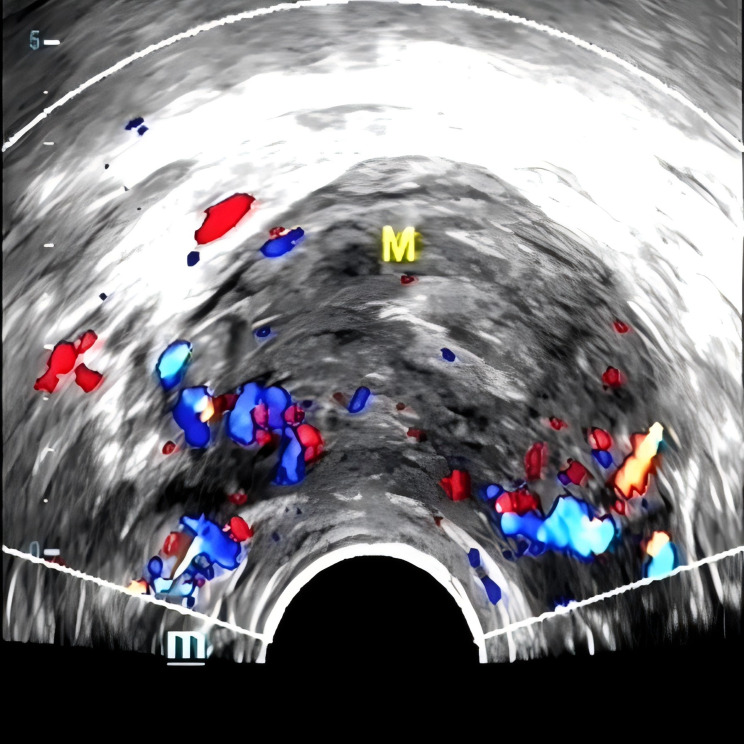
Hysteroscopic myomectomy is the first-line treatment for the removal of submucosal myoma in women facing fertility requirements. However, in the face of large diameter type 2 submucosal myoma, patients are at greater risk of complications such as uterine perforation and fluid overload during hysteroscopy. When the diameter of type 2 submucous myoma is greater than 4cm, the three-phase treatment of high intensity focused ultrasound (HIFU), drugs and hysteroscopy is effective and safe. We shared a case of a 30-year-old non-pregnant woman, who had a history of uterine submucous myoma for more than 4 years with symptoms of heavy menstruation, prolonged menstruation and secondary severe anemia. The patient's initial pelvic magnetic resonance results suggested a type 2 uterine submucous myoma with a diameter of more than 4cm. We first performed HIFU on the patient, followed by the patient's oral intake of mifepristone tablets for 3 months, and prior to hysteroscopic surgery, the patient's fibroid type was shifted to type 0, and finally successfully completed hysteroscopic myomectomy (HM). Finally, we conclude that when the diameter of type 2 submucosal myoma exceeds 4 cm, preoperative application of HIFU combined with drug treatment should be considered to maximize the reduction of fibroids, improve symptoms such as anemia and dysmenorrhea, reduce the time required for hysteroscopic surgery, and improve the safety of surgery.
Keywords: high intensity focused ultrasound; hysteroscopic myomectomy; mifepristone; submucous myoma of uterus; uterine fibroid.
© 2025 Li et al.
Conflict of interest statement
Junjie Li is now affiliated with Traditional Chinese Medicine Department, Hunan University of Medicine General Hospital, Hunan, Huaihua, 418000, People’s Republic of China. All authors declare that there is no conflict of interest in this study.
Figures
References
-
- American Association of Gynecologic Laparoscopists (AAGL): Advancing Inimally Invasive Gynecology Worldwide. AAGL practice report: practice guidelines for the diagnosis and management of submucous leiomyomas. J Minim Invasive Gynecol. 2012;19(2):152–171. doi: 10.1016/j.jmig.2011.09.005 - DOI - PubMed
-
- Munro MG, Critchley HOD, Fraser IS. FIGO menstrual disorders committee. The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions [published correction appears in Int J Gynaecol Obstet. 2019 Feb;144(2):237]. Int J Gynaecol Obstet. 2018;143(3):393–408. doi: 10.1002/ijgo.12666 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
