

Serum Cytokeratin 18 and Fragment as Biomarkers for Severity and Prognosis in Acute Exacerbation of Chronic Obstructive Pulmonary Disease
- PMID: 40789785
- PMCID: PMC12339617
- DOI: 10.1007/s00408-025-00841-3
Serum Cytokeratin 18 and Fragment as Biomarkers for Severity and Prognosis in Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Abstract
Background: Cytokeratin (CK)18 is present in the bronchi and alveolar epithelium of the lung, and its cleavage product, CK-18M30, serves as a biological marker of apoptosis. However, the specific roles of CK-18 and CK-18M30 in acute exacerbation of chronic obstructive pulmonary disease (AECOPD) remain unclear.
Methods: This study enrolled 289 patients with AECOPD who met the inclusion criteria. Demographic information and clinical characteristics of the patients were documented. A 3-year follow-up period was implemented to evaluate acute exacerbations and mortality. Serum CK-18 and CK-18M30 concentrations were measured using enzyme-linked immunosorbent assays.
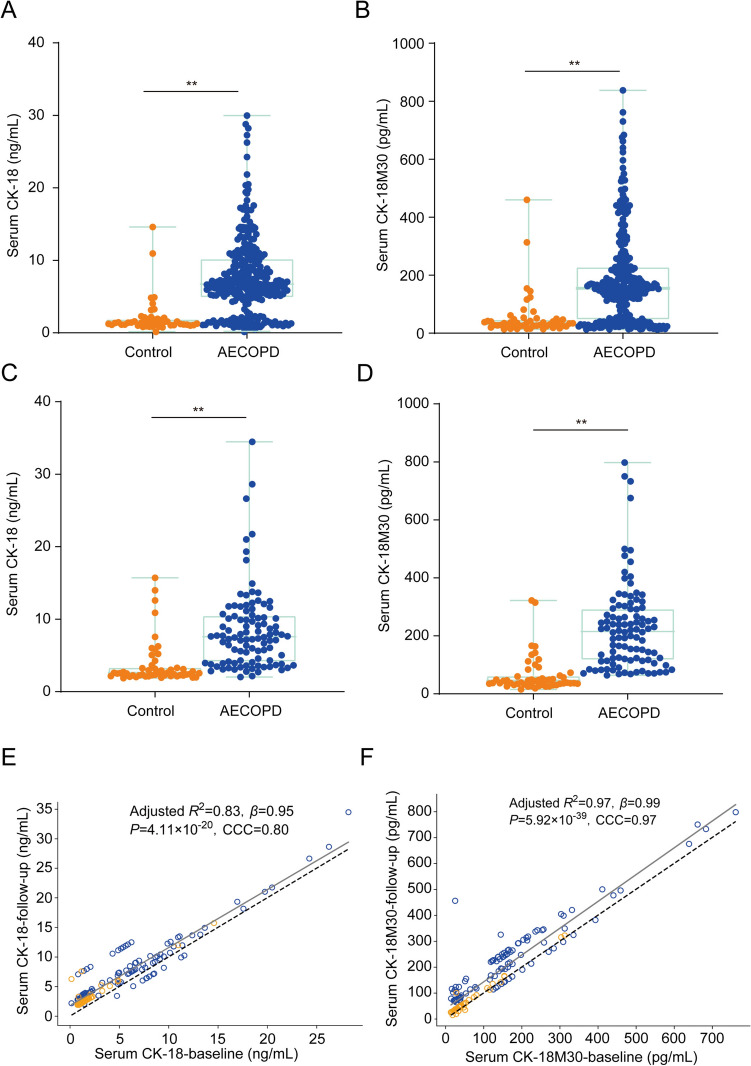
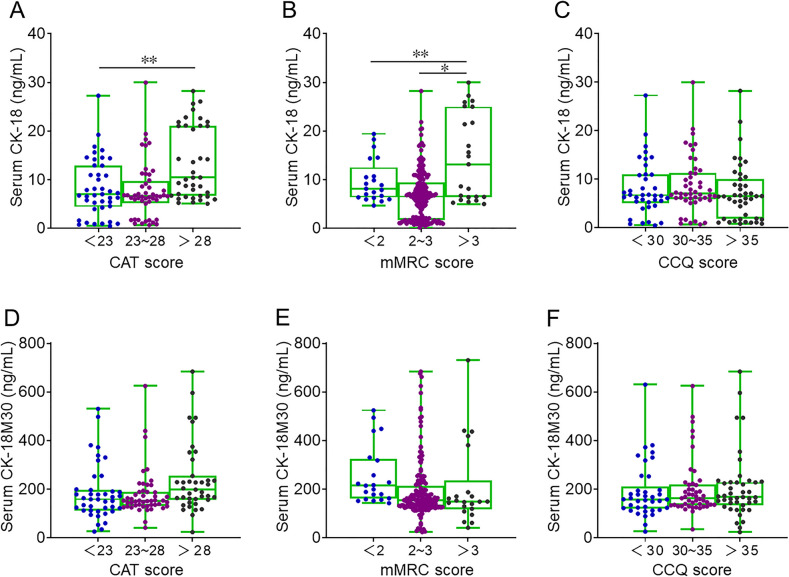
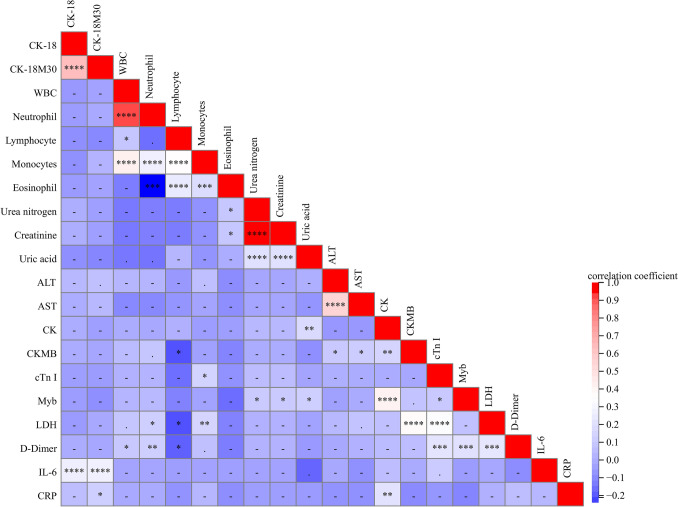
Results: Serum concentrations of CK-18/CK-18M30 at admission in patients with AECOPD were higher than those in the control group. As severity increased, serum CK-18/CK-18M30 levels increased progressively in AECOPD patients. Pearson's correlation analysis revealed that serum CK-18/CK-18M30 concentrations were positively correlated with several clinical parameters. Linear and logistic regression models demonstrated positive correlations between serum CK-18 and CK-18M30 levels at admission and severity scores. Furthermore, higher serum CK-18/CK-18M30 levels at admission were associated with increased frequency of death and acute exacerbation in patients with AECOPD within 3 years.
Conclusion: Serum CK-18/CK-18M30 levels at admission were positively correlated with severity and poor prognosis in patients with AECOPD within 3 years. Therefore, serum CK-18 and CK-18M30 concentrations may serve as novel diagnostic and prognostic biomarkers for patients with AECOPD.
Keywords: AECOPD; CK-18M30; Cohort study; Cytokeratin 18; Prognosis; Severity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing Interests: The authors declare no competing interests. Ethical Approval: This study was performed in compliance with the Declaration of Helsinki and was approved by the Ethics Committee of the Second Affiliated Hospital of Anhui Medical University (YX2021-146). Consent to Participate: Oral agreement or consent forms were obtained from patients or patients’ next of kin. Consent for Publication: Not applicable.
Figures
References
-
- Boers E, Barrett M, Su JG, Benjafield AV, Sinha S, Kaye L, Zar HJ, Vuong V, Tellez D, Gondalia R, Rice MB, Nunez CM, Wedzicha JA, Malhotra A (2023) Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw Open 6(12):e2346598. 10.1001/jamanetworkopen.2023.46598 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 82270071/National Natural Science Foundation of China
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- 2023AH030117/University Natural Science Research Project of Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- AHWJ2021b091/Scientific Research of Health Commission in Anhui Province
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- JKS2022007/Research Funds of the Center for Big Data and Population Health of IHM
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 202204295107020014/Anhui Provincial Clinical Research Transformation Project
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
- 2022AH040098/the University Natural Science Research Project of Anhui Province
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
