

Estimated glomerular filtration rate, albuminuria, and risk of infection: a collaborative meta-analysis of individual participant data
- PMID: 40791893
- PMCID: PMC12337016
- DOI: 10.1016/j.eclinm.2025.103372
Estimated glomerular filtration rate, albuminuria, and risk of infection: a collaborative meta-analysis of individual participant data
Abstract
Background: Infections are a major cause of hospitalization in people with chronic kidney disease (CKD), with incidence similar to cardiovascular disease, yet the risk of infection has not been systematically studied across stages of CKD.
Methods: We conducted a meta-analysis of individual participant data including 1,246,912 individuals across 47 cohorts in the CKD Prognosis Consortium, with information on estimated glomerular filtration rate based on serum creatinine (eGFRcr) and urinary albuminuria (ACR) (or proteinuria converted to ACR), to examine the association of eGFR and ACR with the risk of hospitalization with infection. Outcomes were ascertained through diagnostic codes on hospital discharge records relevant to acute infections (i.e., upper and lower respiratory tract, urinary tract, skin and soft tissue, musculoskeletal, gastrointestinal tract, genital, nervous system, and cardiovascular system infections, and sepsis). Follow-up was censored on December 31, 2019 or on the last date of cohort follow-up, whichever was earlier. Multivariable Cox models were used to estimate hazard ratios (HRs).
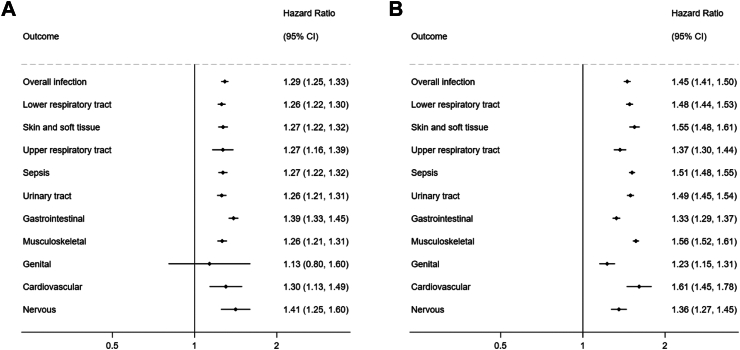
Findings: During follow-up, 170,864 (13.7%) individuals had a hospitalization with infection (IR, 22.0 [IQI, 16.2-31.0] per 1000 person-yrs). In Cox models, compared to eGFRcr 90-104 ml/min/1.73 m2 and ACR <10 mg/g, lower eGFRcr and higher ACR were each independently associated with an increased hazard of infection in a graded manner, including in eGFRcr 60-89 and 45-59 ml/min/1.73 m2 (adjusted HRs [95% CI], 1.09 [1.06-1.13] and 1.39 [1.34-1.45]) and ACR 10-29 and 30-299 mg/g (1.40 [1.33-1.47] and 1.82 [1.72-1.92]). High eGFRcr ≥105 ml/min/1.73 m2 was also associated with the risk of infection (1.22 [1.17-1.26]). Combined, eGFRcr <30 ml/min/1.73 m2 and ACR ≥ 300 mg/g were associated with more than 6-fold higher hazard of infections (6.27 [5.70-6.90]). These findings were consistent across infection subtypes (e.g., HRs for lower respiratory tract infections, 1.26 [1.22-1.30] per -15 ml/min/1.73 m2 in eGFR and 1.48 [1.44-1.53] per 8-fold increase in ACR).
Interpretation: Lower kidney function and higher albuminuria were independently associated with higher risk of infection. The risk was elevated even in mild to moderate CKD, with the highest risk seen in the most advanced stage of CKD. Infection prevention measures should target individuals across all CKD stages.
Funding: US National Kidney Foundation and the National Institute of Diabetes and Digestive and Kidney Diseases.
Keywords: Albuminuria; Chronic kidney disease; Estimated glomerular filtration rate; Infection; Risk.
© 2025 The Author(s).
Conflict of interest statement
Drs. Alencar de Pinho and Stengel have received financial support of the Agence Nationale de la Recherche (France) through the 2010 «Cohortes-Investissements d’Avenir» program (ANR-IA-COH-2012/3731), the 2010 national Programme Hospitalier de Recherche Clinique, and through a public-private partnership with GlaxoSmithKline (GSK) since 2012, Boehringer Ingelheim France since 2022, Novo Nordisk since 2024, Fresenius Medical Care from 2012 to 2024, Vifor France from 2018 to 2023, Sanofi-Genzyme from 2012 to 2015, Baxter and Merck Sharp & Dohme-Chibret (MSD France) from 2012 to 2017, Amgen from 2012 to 2020, Lilly France from 2013 to 2018, Otsuka Pharmaceutical from 2015 to 2020, and AstraZeneca from 2018 to 2021. All grants are made to Paris-Saclay University. Dr. Ärnlöv has served on advisory boards for Astella, AstraZeneca, and Boehringer Ingelheim, and has received lecturing fees from AstraZeneca and Boehringer Ingelheim, all of which are unrelated to the present work. Dr. Bell has received consultancy fees from Astra Zeneca, GSK and Bayer and participated on the Stada UK unrelated to present work. Dr. Carrero received grants to Karolinska Institutet from AstraZeneca, Boehringer, MSD, Astellas, Novonordisk, ViforPharma as well as honoraria from Fresenuis Kabi. Dr. Chang has received grant funding from Novartis, Boehringer-Ingelheim, Bayer, Novo Nordisk, National Kidney Foundation; consulting fees from Amgen serving on the advisory board. Dr. Coresh received grants from NIH. Dr. Grams has received grants from NIH and honoraria from University of Pennsylvania, Columbia University Medical Center, and NephSAP; she also receives support to attend meetings from KDIGO, European Renal Association, University of Pennsylvania, Korean Society of Nephrology, Hong Kong Society of Nephrology, and the Kidney Research Institute; and she has a leadership role in the American Society of Nephrology Publication Committee, Kidney Disease: Improving Global Outcomes (Co-Chair), National Kidney Foundation Scientific Advisory Committee, United States Renal Data System Scientific Advisory Board, Kidney Institute Executive Committee, Clinical Journal of American Society of Nephrology. American Journal of Kidney Diseases, and the Journal of American Society of Nephrology. Dr. Haynes received an institutional grant to support the SHARP trial from Merck Sharp & Dohme and grants from Boehringer Ingelheim, Roche, and Regeneron; he has also served as an unpaid member of the DMC at Eli Lilly. Dr. Lees has received personal lectureship honoraria from Astra Zeneca and consulting fees from Boehringer Ingelheim outside the submitted work. Dr. Matsushita received grants from the NIH and Resolve to Save Lives as well as consulting fees from RhythmX AI, and honoraria from Fukuda Denshi. Dr. Rao received a grant from NIDDK. Dr. Robinson-Cohen received grants from NIDDK. Dr. Ix received grants from NIDDK, NHLBI, and Breakthrough T1D; consulting fees from Bayer and AstraZeneca; and support to attend meetings by the American Society of Nephrology and Kidney Disease: Improving Global Outcomes; and has a leadership role in AlphaYoung; and received equipment or materials from Genentech. All other authors declare no competing interests.
Figures


References
-
- Johansen K.L., Gilbertson D.T., Li S., et al. US renal data system 2023 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2024;83(4S1):A8–A13. - PubMed
-
- James M.T., Laupland K.B., Tonelli M., et al. Risk of bloodstream infection in patients with chronic kidney disease not treated with dialysis. Arch Intern Med. 2008;168(21):2333–2339. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
