

Management of a First Branchial Cleft Fistula in an Adult Patient: A Case Report and Literature Review
- PMID: 40792327
- PMCID: PMC12336603
- DOI: 10.7759/cureus.87756
Management of a First Branchial Cleft Fistula in an Adult Patient: A Case Report and Literature Review
Abstract
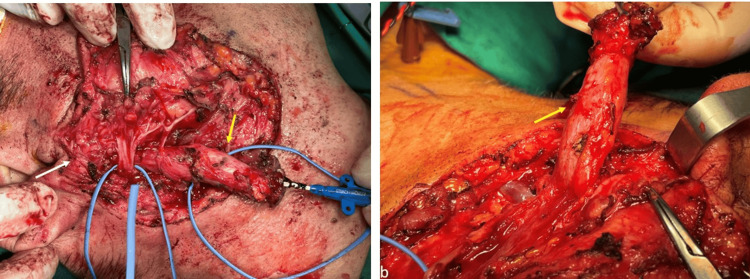
First branchial cleft anomalies (FBCAs) are uncommon congenital malformations that develop due to incomplete closure of the first branchial cleft during embryonic development. They represent a small proportion of all branchial cleft anomalies. These lesions, which may present as cysts, sinuses, or fistulas, pose significant diagnostic and therapeutic challenges due to their nonspecific clinical manifestations and complex anatomical relationships, particularly with the facial nerve and parotid gland. This case report describes a 47-year-old male patient presenting with recurrent infections and purulent discharge in the right preauricular and submandibular regions, later diagnosed as a Work Type II first branchial cleft fistula extending from the external auditory canal (EAC) through the parotid gland to the submandibular skin. Diagnostic evaluation included high-resolution magnetic resonance imaging (MRI) and computed tomography (CT) fistulography, which confirmed the fistula's course and its intimate relation to the facial nerve. Surgical management involved complete excision via a modified Blair incision, retrograde facial nerve dissection, and superficial parotidectomy, with intraoperative neuromonitoring to minimize nerve injury risk. Histopathology revealed a cutaneous fistulous tract lined with stratified squamous epithelium and sparse chronic inflammatory infiltrates. Postoperative recovery was uneventful, with transient House-Brackmann grade II facial nerve palsy resolving within four weeks and no recurrence at the 12-month follow-up. This case is notable for the patient's unusually late presentation in adulthood, contrasting with the typical diagnosis in childhood. A comprehensive literature review highlights the embryological basis, clinical variability, and diagnostic challenges of FBCAs, emphasizing the critical role of preoperative imaging for delineating the fistula's anatomy and planning surgery. Complete surgical excision with facial nerve preservation remains the gold standard, though the procedure is complicated by the lesion's proximity to critical neurovascular structures. Intraoperative neuromonitoring and patient-specific surgical approaches are essential to minimize complications such as facial nerve palsy and recurrence. This case underscores the importance of timely diagnosis, meticulous preoperative planning, and specialized surgical expertise in achieving favorable outcomes for FBCAs, particularly in atypical adult presentations.
Keywords: branchial region; congenital abnormalities; facial nerve; fistula; parotid gland.
Copyright © 2025, Louizakis et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Scientific committee of George Papanikolaou General Hospital of Thessaloniki, Greece issued approval (394, 3.6.2025). Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






References
-
- Branchial cleft and pouch anomalies in childhood: a report of 50 surgical cases. Spinelli C, Rossi L, Strambi S, Piscioneri J, Natale G, Bertocchini A, Messineo A. J Endocrinol Invest. 2016;39:529–535. - PubMed
-
- Clinical manifestations, diagnosis, and management of first branchial cleft fistula/sinus: a case series and literature review. Liu H, Cheng A, Ward BB, Wang C, Han Z, Feng Z. J Oral Maxillofac Surg. 2020;78:749–761. - PubMed
Publication types
LinkOut - more resources
Full Text Sources