

The Effect of Pain on the Relationship Between Triage Acuity and Emergency Department Hospitalization Rate and Length of Stay
- PMID: 40794967
- PMCID: PMC12342432
- DOI: 10.5811/westjem.33600
The Effect of Pain on the Relationship Between Triage Acuity and Emergency Department Hospitalization Rate and Length of Stay
Abstract
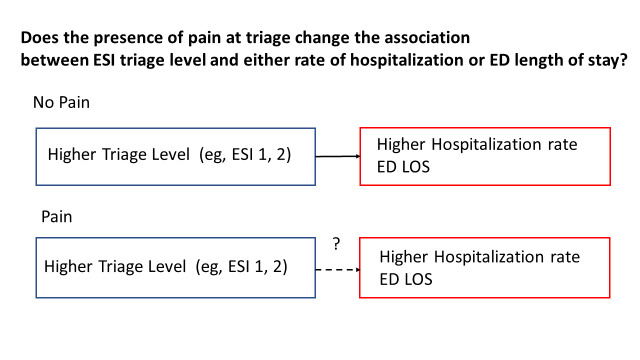
Objectives: Little is known about the effect of pain on the relationship between triage and patient outcomes in United States emergency departments (ED). In this study we aimed to describe pain-associated ED visits and to explore how pain modifies the ability of ED triage to predict patient outcomes (hospitalization and ED length of stay [EDLOS)].
Methods: We obtained data from the National Hospital Ambulatory Medical Care Survey (NHAMCS), 2010-2021. Adult ED visits without missing data on pain score or triage level were included. We assessed pain scores at triage using a numeric rating scale (NRS) of 0-10. We further categorized the NRS scores into no (0), mild (1-3), moderate (4-6), and severe (7-10) pain. The five-level Emergency Severity Index was used for ED triage. The primary outcomes were hospital admission during the ED visit and EDLOS. For the analyses we used descriptive statistics and multivariable regression accounting for NHAMCS's complex survey design.
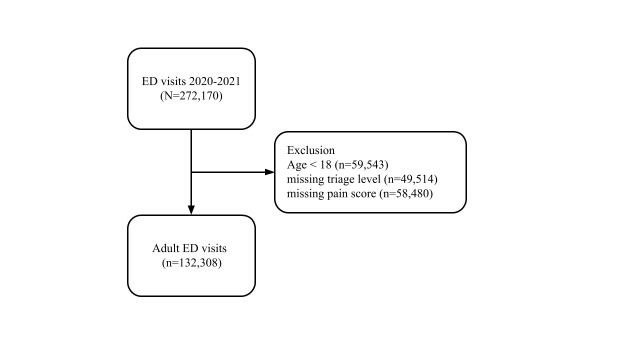
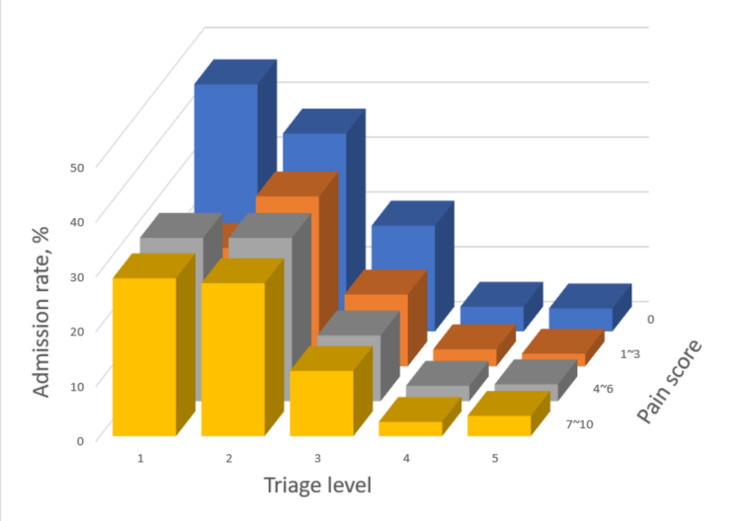
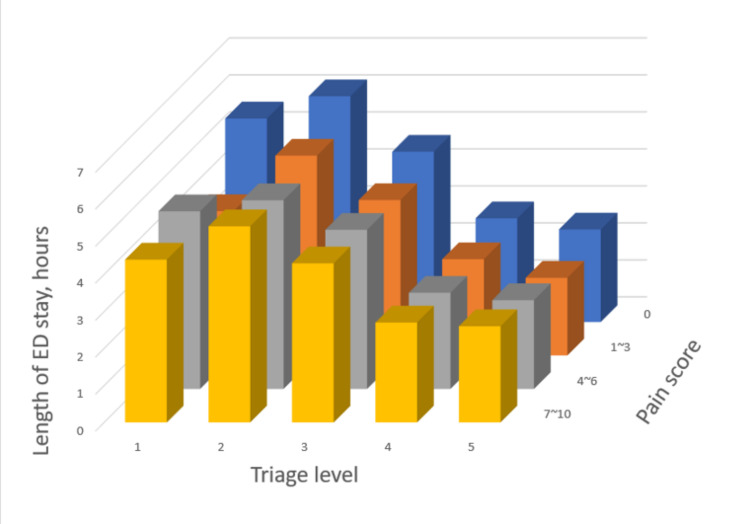
Results: Over the 12-year study period, there were 132,308 adult ED visits (representing 773,000,000 ED visits nationwide). Approximately 50% were triaged to level 3, followed by 30% to level 4. Approximately 45% reported severe pain, 21% moderate pain, 9% mild pain, and 25% no pain. Triage level 1 was associated with the highest rate of hospitalization (35%), with a gradual decrease in hospitalization rate from levels 2 to 4. Triage level 2 was associated with the longest mean EDLOS (5.6 hours), with a gradual decrease in EDLOS from levels 3 to 5. When stratified by pain intensity, the pattern of hospitalization altered in the mild and moderate pain groups. In these two pain-intensity groups, triage level 1 was associated with lower-than-expected odds of hospitalization, a 31% reduction suggested by the interaction term (adjusted odds ratio 0.69; 95% confidence interval .51-.92, P = .01). By contrast, the pattern of EDLOS persisted across all pain-intensity groups.
Conclusion: Mild and moderate levels of pain intensity appear to negatively impact the ability of triage to predict hospitalization, resulting in overtriage among patients in these two pain-intensity groups. Pain intensity in the ED should be carefully evaluated to avoid overtriage and ensure the appropriate allocation of resources.
Figures
Similar articles
-
Risk Factors for Hospital Admissions Among Emergency Department Patients: From Triage to Admission.West J Emerg Med. 2025 Feb 25;26(3):513-522. doi: 10.5811/westjem.21263. West J Emerg Med. 2025. PMID: 40562001 Free PMC article.
-
Emergency Severity Index Version 4 and Triage of Pediatric Emergency Department Patients.JAMA Pediatr. 2024 Oct 1;178(10):1027-1034. doi: 10.1001/jamapediatrics.2024.2671. JAMA Pediatr. 2024. PMID: 39133479 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Assessment and support during early labour for improving birth outcomes.Cochrane Database Syst Rev. 2017 Apr 20;4(4):CD011516. doi: 10.1002/14651858.CD011516.pub2. Cochrane Database Syst Rev. 2017. PMID: 28426160 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
References
-
- Marco CA, Kanitz W, Jolly M. Pain scores among emergency department (ED) patients: comparison by ED diagnosis. J Emerg Med. 2013;44(1):46–52. - PubMed
-
- Davis S, Ju C, Marchandise P, et al. Impact of pain assessment on Canadian Triage and Acuity Scale prediction of patient outcomes. Ann Emerg Med. 2022;79(5):433–40. - PubMed
-
- Daoust R, Paquet J, Bailey B, et al. Vital signs are not associated with self-reported acute pain intensity in the emergency department. CJEM. 2016;18(1):19–27. - PubMed
-
- Levy N, Sturgess J, Mills P. “Pain as the fifth vital sign” and dependence on the “numerical pain scale” is being abandoned in the US: Why? Br J Anaesth. 2018;120(3):435–8. - PubMed
-
- Karcioglu O, Topacoglu H, Dikme O, et al. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical