

The role of statins during pregnancy on maternal risk of preeclampsia: a systematic review and meta-analysis
- PMID: 40796817
- PMCID: PMC12341335
- DOI: 10.1186/s12884-025-07967-5
The role of statins during pregnancy on maternal risk of preeclampsia: a systematic review and meta-analysis
Abstract
Background: Preeclampsia is a leading cause of maternal and perinatal morbidity and mortality, characterized by angiogenic imbalance and systemic dysfunction after 20 weeks of gestation. Statins, particularly pravastatin, have showed potential in prevention due to their anti-inflammatory and endothelial-protective properties, though safety in pregnancy remains uncertain. This systematic review and meta-analysis aimed to evaluate the efficacy of statins and their association with maternal risk of preeclampsia.
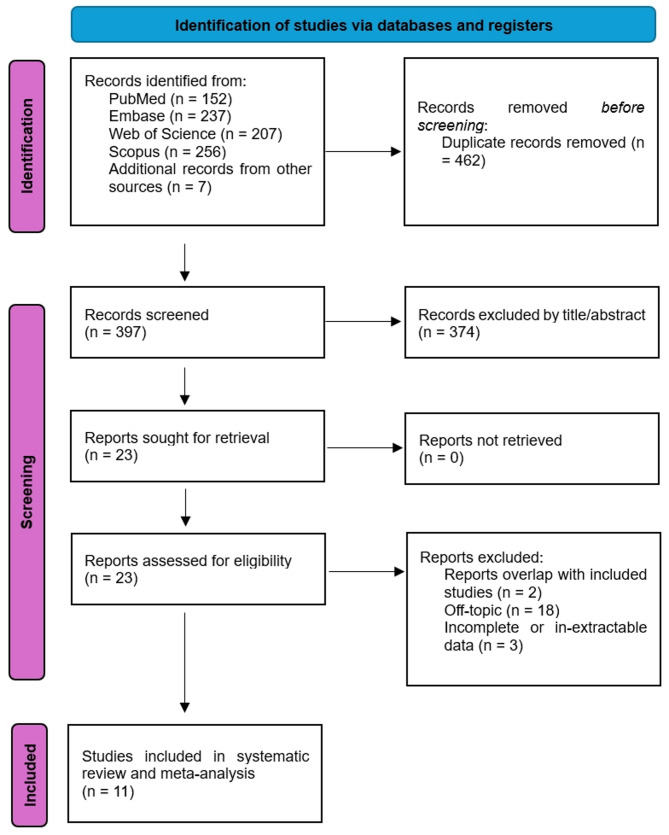
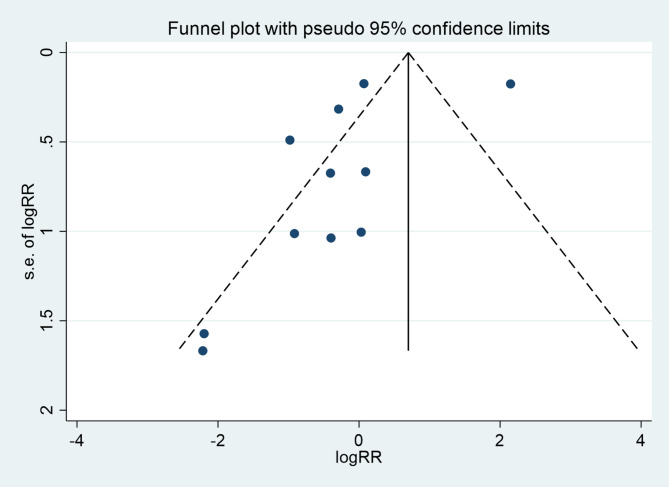
Methods: Two independent reviewers systematically searched data from PubMed, Scopus, Web of Science, Cochrane, and Embase databases until December 2024 for studies evaluating statins for prevention of pre-eclampsia. Those healthy pregnant women who did not develop preeclampsia were assessed as comparators. Letters, comments, case reports, and reviews were excluded. Newcastle-Ottawa Scale (NOS) were used for assessing case-control and cohort studies. The Cochrane Risk of Bias 2.0 (RoB 2.0) were adopted for evaluating randomized trials. The primary outcome was preeclampsia. Secondary outcomes included the hypertensive disorders of pregnancy (HDP), preterm labor (PTB), neonatal birth defects, and neonatal intensive care unit (NICU) admission. The random-effects method (REM) or fixed-effects method (FEM) were employed depending on the heterogeneity. Sub-group analysis was performed to identify the source of heterogeneity. The publication bias was assessed via the funnel plot, Egger's and Begg's tests. The leave-one-out sensitivity analysis were also performed. The RevMan 5.3 and Stata 16.0 were the main software used for data extraction and analysis.
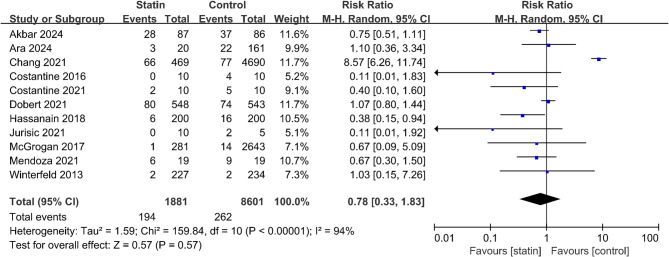
Results: 11 different studies covering 10,482 pregnant participants, with 456 diagnosed with preeclampsia. Results showed a pooled risk ratio (RR) of 0.78 (95% CI: 0.33 to 1.83, p = 0.57), indicating that statin use during pregnancy was not significantly associated with a reduced risk of preeclampsia. Heterogeneity among studies was high (I² = 94%, p < 0.05), suggesting variability in study populations, dosages, and statin types. The second outcomes also showed insignificant statistical difference. Sub-group analysis implied early initiation of statins may reduce preeclampsia risk during pregnancy. Sensitivity analysis revealed that no single study had significant impact on the overall effect.
Conclusion: Due to significant heterogeneity, current evidence is insufficient to establish a definitive protective role for statins in preventing preeclampsia during pregnancy. While subgroup findings suggest that early initiation may be associated with reduced risk, these observations should be interpreted with caution and require confirmation in future high-quality trials.
Trial registration: The study protocol was registered with PROSPERO (No. CRD42024601996).
Keywords: Gestational hypertension; Hypertensive disorders of pregnancy; Preeclampsia; Pregnancy complication; Statins.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Dimitriadis E, Rolnik DL, Zhou W, Estrada-Gutierrez G, Koga K, Francisco RPV, Whitehead C, Hyett J, da Silva Costa F, Nicolaides K, et al. Pre-eclampsia. Nat Rev Dis Primers. 2023;9(1):8. - PubMed
-
- Melchiorre K, Giorgione V, Thilaganathan B. The placenta and preeclampsia: villain or victim? Am J Obstet Gynecol. 2022;226(2S):S954–62. - PubMed
-
- Provinciatto H, Barbalho ME, Almeida J, Provinciatto A, Philip CE. The role of Pravastatin in preventing preeclampsia in high-risk pregnant women: a meta-analysis with trial sequential analysis. Am J Obstet Gynecol MFM. 2024;6(2):101260. - PubMed
-
- Gajzlerska-Majewska W, Bomba-Opon DA, Wielgos M. Is pravastatin a milestone in the prevention and treatment of preeclampsia? J Perinat Med. 2018;46(8):825–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
