

Prognostic utility of somatosensory evoked potentials in supratentorial hemorrhage-induced prolonged disorders of consciousness
- PMID: 40796886
- PMCID: PMC12344912
- DOI: 10.1186/s40001-025-03027-y
Prognostic utility of somatosensory evoked potentials in supratentorial hemorrhage-induced prolonged disorders of consciousness
Abstract
Purpose: To evaluate the prognostic value of somatosensory evoked potentials (SEPs) in predicting functional outcomes in patients with prolonged disorders of consciousness (PDOC) secondary to severe supratentorial intracerebral hemorrhage (ICH).
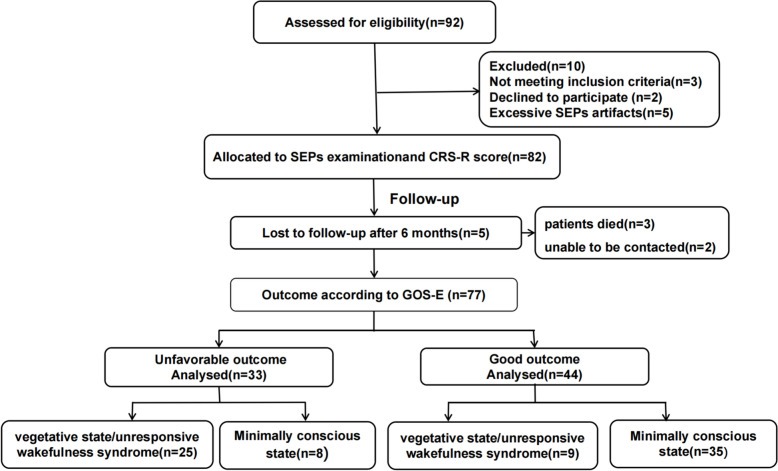
Methods: From August 2023 to August 2024, 77 patients with PDOC secondary to supratentorial intracerebral hemorrhage were prospectively enrolled from Critical Care Rehabilitation Department of Nanjing Jiangning Hospital. Within one week of enrollment, all patients were assessed using the Chinese Coma Recovery Scale-Revised (CRS-R) score, short-latency somatosensory evoked potentials (SLSEPs), and middle-latency somatosensory evoked potentials (MLSEPs). Patients were followed for 6 months, with outcomes classified using the Extended Glasgow Outcome Scale (GOSE). Based on GOSE scores, patients were categorized into good outcome groups (GOSE score ≥ 4) and poor outcome groups(GOSE score < 4).
Results: A total of 77 PDOC patients were included in the study. After 6 months of follow-up, 44 patients (57.14%) demonstrated good outcomes, while 33 (42.86%) had poor outcomes. The absence of N20 and N60 potentials showed significant differences between outcome groups (P < 0.05). Multivariate logistic regression analysis revealed that baseline CRS-R score (OR = 1.51, P = 0.009), N20-P25 mean amplitude (OR = 6.58, P = 0.003), and P45-N60 mean amplitude (OR = 11.99, P = 0.02) were significant predictors of good outcomes in all patients. In the minimally conscious state (MCS) subgroup, the CRS-R score at baseline (OR = 1.38), N20-P25 mean amplitude (OR = 1.85), and P45-N60 mean amplitude (OR = 16.01) significantly predicted outcomes; receiver operating characteristic analysis demonstrated that both N20-P25 mean amplitude (AUC = 0.82, cutoff 1.55 μV, sensitivity = 86.4%, specificity = 69.0%) and P45-N60 mean amplitude (AUC = 0.70, cutoff 0.43 μV, sensitivity = 79.1%, specificity = 71.4%) effectively predicted good outcomes (GOSE ≥ 4) in all patients. Notably, in the MCS subgroup, P45-N60 mean amplitude showed exceptional predictive performance (AUC = 0.93, cutoff 0.38 μV), with 88.6% sensitivity and 100% specificity. Pearson correlation analysis indicated that N20-P25 mean amplitudes significantly correlated with CRS-R score improvement after 6 months (P < 0.05) in all patients and the MCS subgroup. The P45-N60 mean amplitude showed a significant correlation with CRS-R score improvement only in the MCS subgroup (P < 0.05).
Conclusion: Quantitative analysis of SEPs offers clinically significant prognostic value in PDOC following supratentorial ICH. Notably, MLSEPs' demonstrate particularly precise predictive capabilities for MCS patients.
Keywords: Coma recovery scale-revised score; Disorders of consciousness; Prognosis; Somatosensory evoked potentials; Supratentorial cerebral hemorrhage.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki II and good clinical practice guidelines. The study protocol was approved by the Institutional Review Board of Jiangning Hospital Affiliated to Nanjing Medical University (Approval Code: 2022-03-047-k01; Date: 2023-02-22). Written informed consent was obtained from legal guardians of all participants. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
N20-P25 Amplitude can Predict Awakening from Coma.Neurocrit Care. 2025 Aug 11. doi: 10.1007/s12028-025-02335-9. Online ahead of print. Neurocrit Care. 2025. PMID: 40789803
-
Blink reflex as a prognostic indicator for patients with prolonged disorders of consciousness: a prospective case-control study.BMJ Open. 2025 Aug 31;15(8):e099594. doi: 10.1136/bmjopen-2025-099594. BMJ Open. 2025. PMID: 40887124
-
A novel nomogram for predicting prolonged disorders of consciousness in severe supratentorial hypertensive intracerebral hemorrhage patients.Sci Rep. 2025 Jul 17;15(1):25911. doi: 10.1038/s41598-025-11798-x. Sci Rep. 2025. PMID: 40676114 Free PMC article.
-
Assessment scales for disorders of consciousness: evidence-based recommendations for clinical practice and research.Arch Phys Med Rehabil. 2010 Dec;91(12):1795-813. doi: 10.1016/j.apmr.2010.07.218. Arch Phys Med Rehabil. 2010. PMID: 21112421
-
Surgery for spontaneous supratentorial intracerebral haemorrhage.Cochrane Database Syst Rev. 2025 Jul 17;7(7):CD015387. doi: 10.1002/14651858.CD015387.pub2. Cochrane Database Syst Rev. 2025. PMID: 40673401 Free PMC article.
References
-
- Giacino JT, Fins JJ, Laureys S, et al. Disorders of consciousness after acquired brain injury: the state of the science. Nat Rev Neurol. 2014. 10.1038/nrneurol.2013.279. - PubMed
-
- Giacino JT, Ashwal S, Childs N, et al. The minimally conscious state: definition and diagnostic criteria. Neurology. 2002. 10.1212/wnl.58.3.349. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
