

How to Evaluate Hospital Care in the Dying Phase-Development of a Data Extraction Tool for Retrospective Medical Record Analysis
- PMID: 40799077
- PMCID: PMC12344475
- DOI: 10.1111/jep.70174
How to Evaluate Hospital Care in the Dying Phase-Development of a Data Extraction Tool for Retrospective Medical Record Analysis
Abstract
Background: Hospitals are the most common place of death in European countries, including Germany, where nearly half of the population dies in hospitals, mostly outside specialised palliative care wards. At the same time, quality of hospital care in the dying phase is reported as poor. Although existing (inter-)national guidelines provide outcome variables, their evaluation of implementation is lacking. This study aims to develop and test a structured tool for data extraction from medical records (MRs) to evaluate hospital care in the dying phase. The provision of such a tool can help to identify needs for improvement of care.
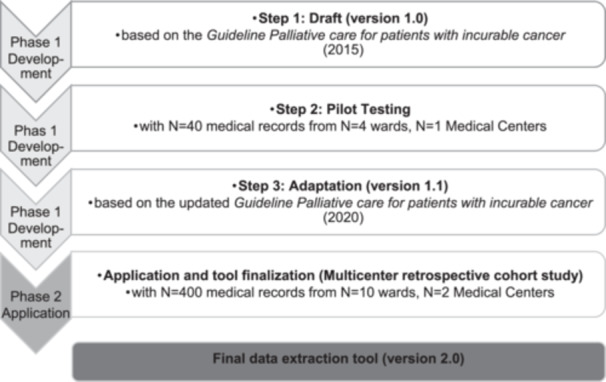
Methods: We developed a data extraction tool by operationalizing recommendations for the dying phase of the evidenced-based German National Palliative Care Guideline. The tool was used to extract notes from MRs of n = 400 deceased patients of 10 general wards and intensive care units at two University Medical Centres. We analysed the tool's information density and content validity. Descriptive statistics were calculated as frequencies and percentages.
Results: The final tool consists of 39 variables in six domains. Initially, 55 variables were derived from guideline recommendations. With regard to content validity, notes for 37 (67%) variables could be extracted from the MRs, while 16 variables were removed due to poor or unclear documentation. Two additional variables were identified inductively and included in the final tool. Notes could be extracted for all domains, while information density (% of MR with notes) varied: (1) Dying process and death (n = 380, 95.0%), (2) Medication and interventions (N = 323, 80.7%), (3) Information and involvement of patients and informal caregivers (n = 155, 38.8%), (4) Symptom assessment (n = 105, 26.3%), (5) Involvement of specialised palliative care (n = 78, 19.5%), (6) Goals-of-care (n = 76, 19.0%). Variation in documentation can reflect differences in care provision or recording practices, suggesting a need for documentation standards.
Conclusion: The tool enables a structured retrospective analysis of guideline-recommended aspects of care in the dying phase in MRs, applicable to both general wards and intensive care units. It can support quality improvement by identifying documentation gaps and areas of care improvement, and can contribute to target interventions in different hospital settings. To obtain a comprehensive understanding of the care provided, MR analysis should be combined with other methods and perspectives and tested in other settings.
Trial registration: The study is registered in the German Clinical Trials Register (DRKS00025405).
Keywords: dying in hospital; dying phase; medical record analysis; palliative care; quality of care.
© 2025 The Author(s). Journal of Evaluation in Clinical Practice published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Radbruch L. and Payne S., “White Paper on Standards and Norms for Hospice and Palliative Care in Europe: Part 2,” European Journal of Palliative Care 17, no. 1 (2010): 22–33.
-
- Statistisches Bundesamt , Diagnosedaten der Patienten und Patientinnen in Krankenhäusern (einschl. Sterbe‐ und Stundenfälle) aus 2016 Wiesbaden 2017. [updated 20.11.2017], https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Kranken....
-
- Zich K. and Sydow H., Sterbeort Krankenhaus – Regionale Unterschiede und Einflussfaktoren (Bertelsmann‐Stiftung, 2015).
-
- Prütz F. and Saß A.‐C., “Daten zur Palliativversorgung in Deutschland,” Bundesgesundheitsblatt ‐ Gesundheitsforschung ‐ Gesundheitsschutz 60, no. 1 (2017): 26–36. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
