

Upper Extremity Cast Application
- PMID: 40799459
- PMCID: PMC12341709
- DOI: 10.1016/j.jposna.2025.100240
Upper Extremity Cast Application
Abstract
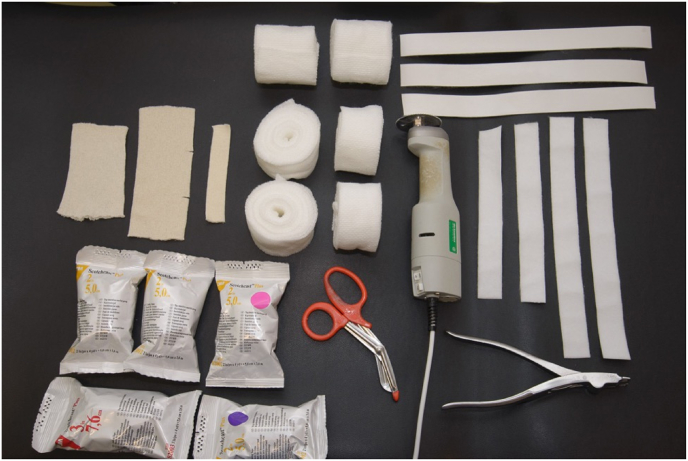
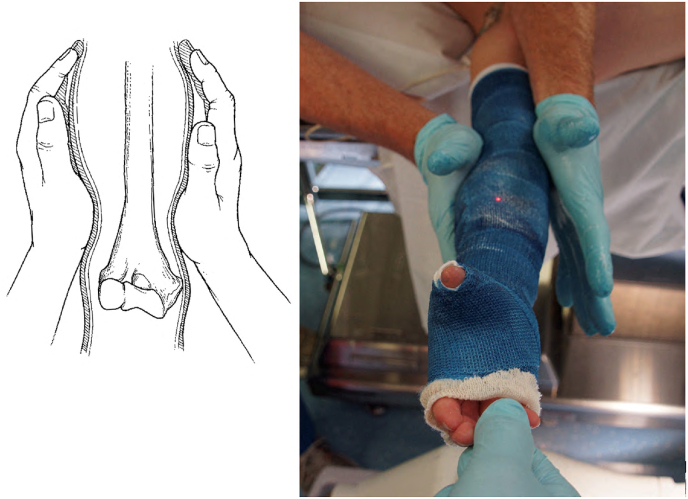
This chapter aims to provide a comprehensive review of the techniques and challenges associated with applying upper extremity casts in pediatric patients. The chapter, along with its accompanying figures and video clips, serves as an introductory guide to pediatric orthopaedic cast application for trainees. Generally, casts are used to preserve appropriate alignment rather than to create improved alignment. In cases of nondisplaced fractures or those with acceptable alignment, the role of the cast is to maintain that alignment until healing occurs. For fractures with unacceptable alignment, reducing them to an acceptable position is necessary while the cast is utilized to maintain proper alignment. For challenging fractures that are difficult to keep aligned, have displaced intraarticular components, or are length-unstable, surgical intervention is recommended, followed by casting for immobilization after surgery. This chapter reviews the indications, application, techniques, and pitfalls of short arm, thumb spica, mitten, ulnar gutter, long arm, and hanging arm casts.
Key concepts: (1)The cast index is a valuable measure that impacts the rates of loss of reduction in distal radius fractures.(2)Molds are important not only for maintaining fracture reduction but also for keeping the cast in position and preventing slippage.(3)Along with using a cast saw to split fiberglass casts, a cast splitter should be employed to ensure proper bivalving.
Keywords: Long arm cast; Mitten cast; Short arm cast; Thumb spica cast.
© 2025 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures





















References
-
- Liu D.S., Murray M.M., Bae D.S., May C.J. Pediatric and adolescent distal radius fractures: current concepts and treatment recommendations. J Am Acad Orthop Surg. 2024;32:e1079–e1089. - PubMed
-
- Perry D.C., Achten J., Knight R., Appelbe D., Dutton S.J., Dritsaki M., et al. Immobilisation of torus fractures of the wrist in children (FORCE): a randomised controlled equivalence trial in the UK. Lancet. 2022;400:39–47. - PubMed
-
- Perry D.C., Gibson P., Roland D., Messahel S. What level of immobilisation is necessary for treatment of torus (buckle) fractures of the distal radius in children? Bmj. 2021;372 - PubMed
-
- Gelberman R.H., Szabo R.M., Mortensen W.W. Carpal tunnel pressures and wrist position in patients with Colles' fractures. J Trauma Inj Infect Crit Care. 1984;24:747–749. - PubMed
-
- Alemdarolu K.B., Iltar S., Cimen O., Uysal M., Alagöz E., Atlihan D. Risk factors in redisplacement of distal radial fractures in children. J Bone Jt Surg. 2008;90:1224–1230. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
