

An Innovative Technique of Revision Surgery for Distal Junctional Failure
- PMID: 40799862
- PMCID: PMC12340299
- DOI: 10.7759/cureus.87802
An Innovative Technique of Revision Surgery for Distal Junctional Failure
Abstract
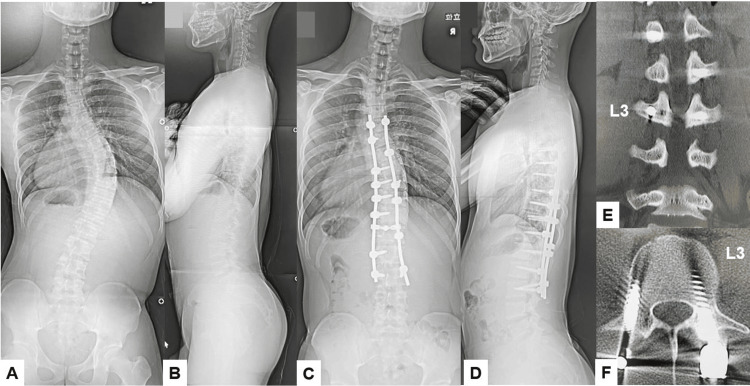
Distal junctional kyphosis (DJK) or the adding-on phenomenon is one of the most challenging complications following long fusion for adolescent idiopathic scoliosis (AIS) or adult spinal deformity (ASD). Among these complications, distal junctional failure (DJF) is defined as a condition requiring revision surgery due to severe symptoms such as intense low back pain, myelopathy, and difficulty in standing and walking. Three patients developed severe lower back pain due to DJF, and two patients underwent revision surgery with a new technique. Surgical outcomes, surgical time, intraoperative blood loss, and operative complications were evaluated. Two patients underwent revision surgery with a novel method for revising distal screw loosening without excessive distal extension. There was no complication, and two patients had solid bony fusion at a two-year follow-up. The revision surgery for type 1 DJK can be challenging because the conventional pedicle screw technique is not feasible for the lower instrumented vertebra, and a more extended distal fusion is required. The adoption of O-arm-guided transdiscal screw fixation has significant clinical implications. This technique also increases accuracy in screw placement, mitigating the risks associated with traditional revision methods and preserving motion segments.
Keywords: c-arm free; distal junctional failure; navigation; reoperation; transdiscal screw.
Copyright © 2025, Tanaka et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Ethics Committe of Okayama Rosai Hospital issued approval 543. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures















References
-
- Distal junctional kyphosis of adolescent idiopathic thoracic curves following anterior or posterior instrumented fusion: incidence, risk factors, and prevention. Lowe TG, Lenke L, Betz R, et al. Spine (Phila Pa 1976) 2006;31:299–302. - PubMed
-
- Risk factors for distal junctional failure in long-construct instrumentation for adult spinal deformity. McDonnell JM, Evans SR, Ahern DP, et al. Eur Spine J. 2022;31:3654–3661. - PubMed
-
- Risk of distal junctional kyphosis in Scheuermann's kyphosis is decreased by selecting the LIV as two vertebrae distal to the first lordotic disc. Luzzi A, Sardar Z, Cerpa M, et al. Spine Deform. 2022;10:1437–1442. - PubMed
-
- Selective thoracic fusion with segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis: more than 5-year follow-up. Suk SI, Lee SM, Chung ER, Kim JH, Kim SS. Spine (Phila Pa 1976) 2005;30:1602–1609. - PubMed
-
- Revision surgery in distal junctional kyphosis. Berjano P, Damilano M, Pejrona M, Langella F, Lamartina C. Eur Spine J. 2020;29:86–102. - PubMed
LinkOut - more resources
Full Text Sources