

Laryngeal Tuberculosis Mimicking Laryngeal Carcinoma: A Case Report
- PMID: 40799900
- PMCID: PMC12341445
- DOI: 10.7759/cureus.87828
Laryngeal Tuberculosis Mimicking Laryngeal Carcinoma: A Case Report
Abstract
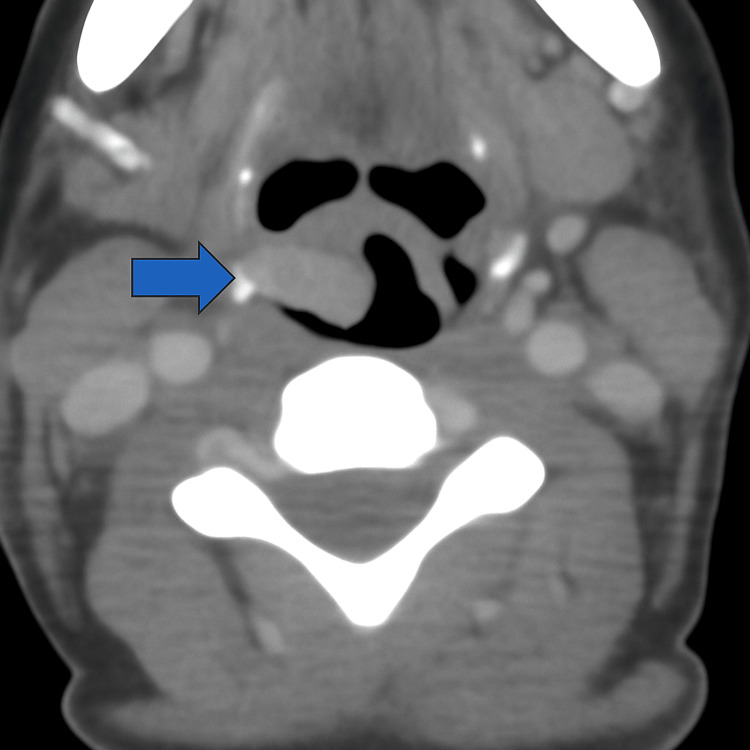
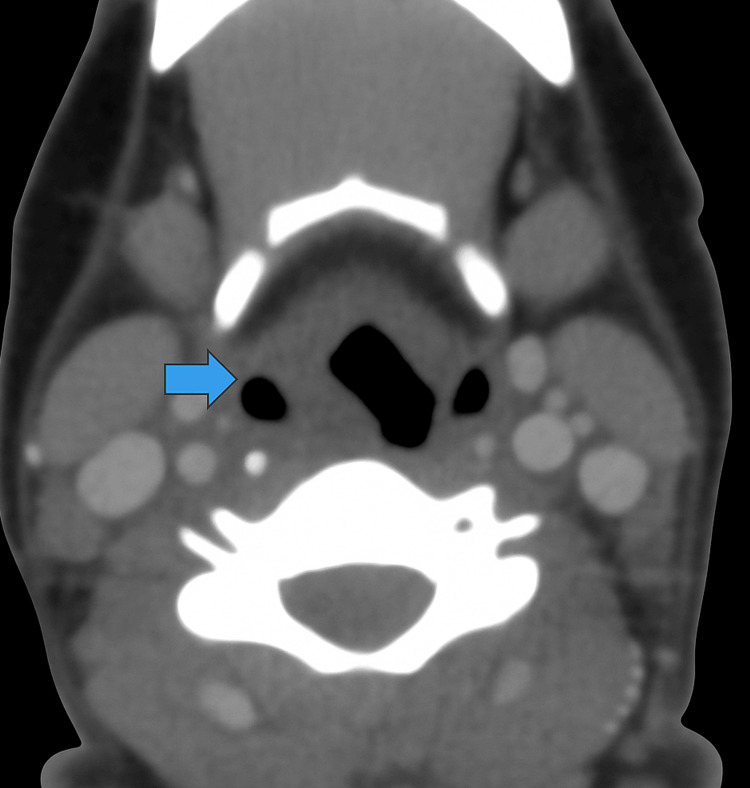
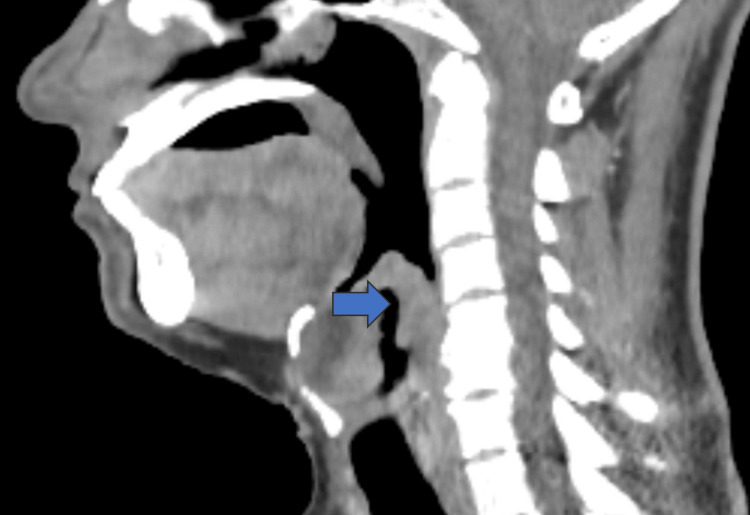
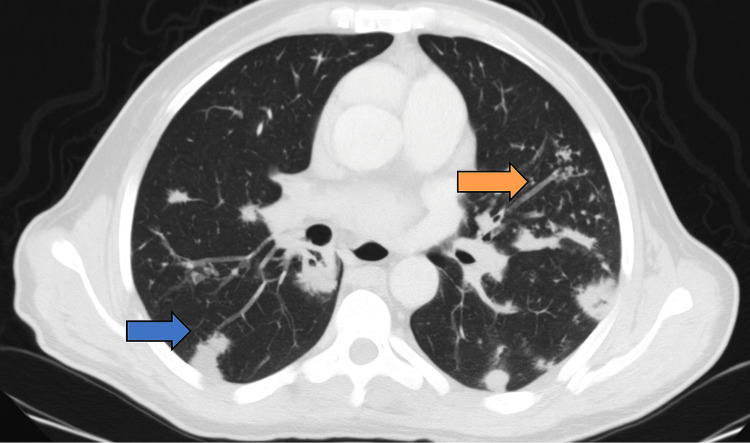
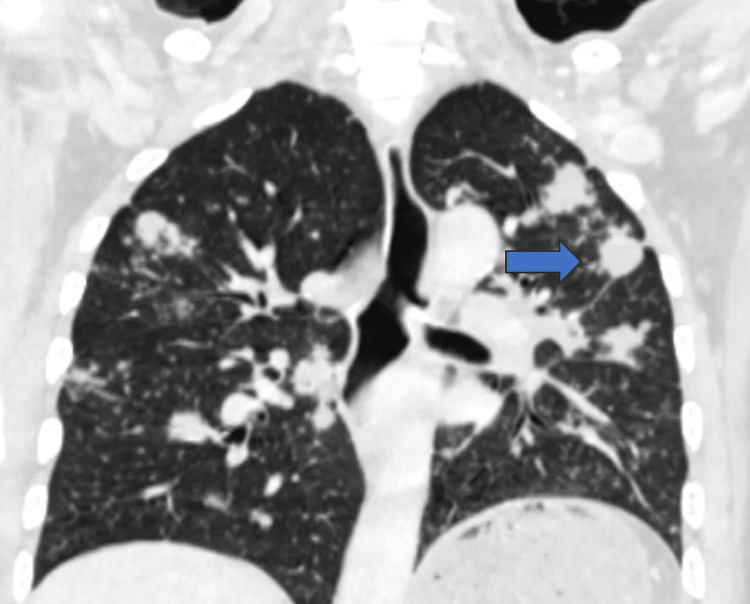
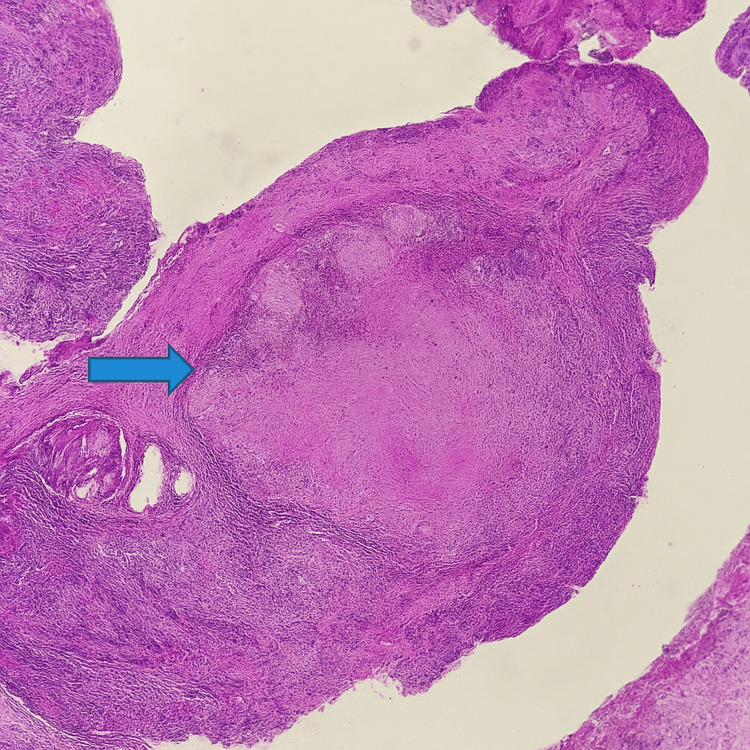
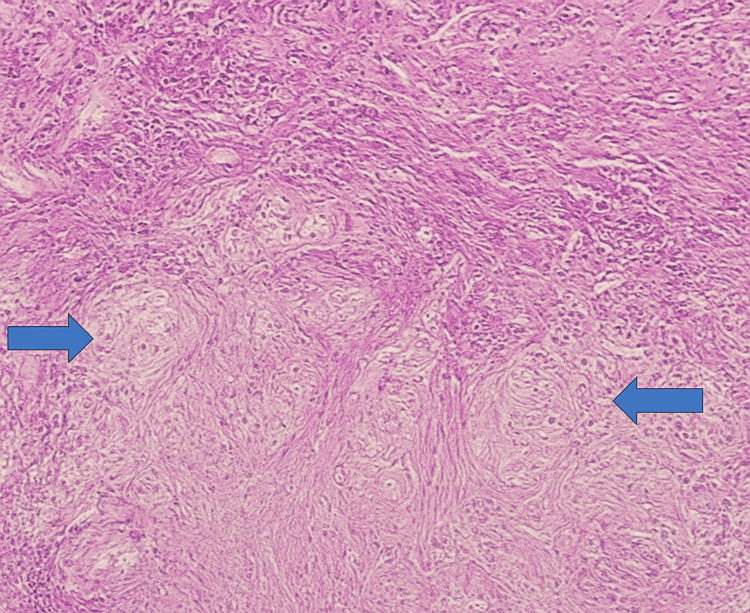
Laryngeal tuberculosis (LTB) is a rare form of extrapulmonary tuberculosis that can clinically and radiologically resemble laryngeal carcinoma, leading to potential misdiagnosis. We report the case of a 53-year-old man with a history of chronic smoking, no known tuberculosis or BCG vaccination, who presented with progressive dyspnea, dysphonia, and significant weight loss. Laryngoscopy revealed ulcerative lesions involving the anterior commissure, right ventricular strip, arytenoid fold, and epiglottis. CT imaging suggested malignancy, but a biopsy confirmed LTB with pulmonary involvement. The patient responded favorably to anti-tuberculous therapy, with near-complete resolution after two months. This case highlights the diagnostic challenge of differentiating LTB from malignancy. Awareness of this rare presentation is essential, especially in tuberculosis (TB)-endemic regions, to avoid unnecessary surgical intervention and ensure prompt medical treatment.
Keywords: caseating granuloma; contrast-enhanced ct; laryngeal carcinoma; laryngeal tuberculosis; mycobacterium tuberculosis.
Copyright © 2025, Yammouri et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Bilateral intraocular masses in a child as a first presentation of disseminated tuberculosis: case report.Ther Adv Ophthalmol. 2025 Jul 13;17:25158414251356373. doi: 10.1177/25158414251356373. eCollection 2025 Jan-Dec. Ther Adv Ophthalmol. 2025. PMID: 40661341 Free PMC article.
-
Case Report: Unveiling the hidden: a rare case of endometrial tuberculosis presenting as peritoneal carcinomatosis.Front Oncol. 2025 Jul 29;15:1607025. doi: 10.3389/fonc.2025.1607025. eCollection 2025. Front Oncol. 2025. PMID: 40799242 Free PMC article.
-
PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer.Cochrane Database Syst Rev. 2014 Nov 13;2014(11):CD009519. doi: 10.1002/14651858.CD009519.pub2. Cochrane Database Syst Rev. 2014. PMID: 25393718 Free PMC article.
-
Xpert® MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance.Cochrane Database Syst Rev. 2018 Aug 27;8(8):CD012768. doi: 10.1002/14651858.CD012768.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Jan 15;1:CD012768. doi: 10.1002/14651858.CD012768.pub3. PMID: 30148542 Free PMC article. Updated.
References
-
- Laryngeal involvement in patients with active pulmonary tuberculosis. Topak M, Oysu C, Yelken K, Sahin-Yilmaz A, Kulekci M. Eur Arch Otorhinolaryngol. 2008;265:327–330. - PubMed
-
- Epiglottic tuberculosis in a patient treated with steroids for Addison's disease. Egeli E, Oghan F, Alper M, Harputluoglu U, Bulut I. Tohoku J Exp Med. 2003;201:119–125. - PubMed
-
- CT findings of laryngeal tuberculosis: comparison to laryngeal carcinoma. Kim MD, Kim DI, Yune HY, Lee BH, Sung KJ, Chung TS, Kim SY. J Comput Assist Tomogr. 1997;21:29–34. - PubMed
-
- Current clinical propensity of laryngeal tuberculosis: review of 60 cases. Lim JY, Kim KM, Choi EC, Kim YH, Kim HS, Choi HS. Eur Arch Otorhinolaryngol. 2006;263:838–842. - PubMed
Publication types
LinkOut - more resources
Full Text Sources