

A new surgical method of vasoepididymostomy for epididymal obstructive azoospermia to improve the success rate in the rat
- PMID: 40800093
- PMCID: PMC12336738
- DOI: 10.21037/tau-2025-91
A new surgical method of vasoepididymostomy for epididymal obstructive azoospermia to improve the success rate in the rat
Abstract
Background: Two-suture longitudinal intussusception vasoepididymostomy (LIVE) surgery has been confirmed by many studies in the treatment of epididymal obstruction; however, the success rate and anastomotic patency rate are not high, which cannot meet the modern human demand for a cure rate for this disease. Based on our preliminary research, we have reason to speculate that the new 2-suture circular intussusception vasoepididymostomy (CIVE) surgery group can greatly improve the anastomosis rate and success rate of treating epididymal obstruction patients. LIVE has become the preferred technique for epididymal and vas deferens anastomosis in North America, Europe, and globally for 22 years. Compared with LIVE, CIVE can greatly improve the anastomosis and success rate of treating epididymal obstruction patients. The aim of this study is to make CIVE the preferred technique for treating epididymal obstruction in North America, Europe, and globally. CIVE ultimately benefits more patients.
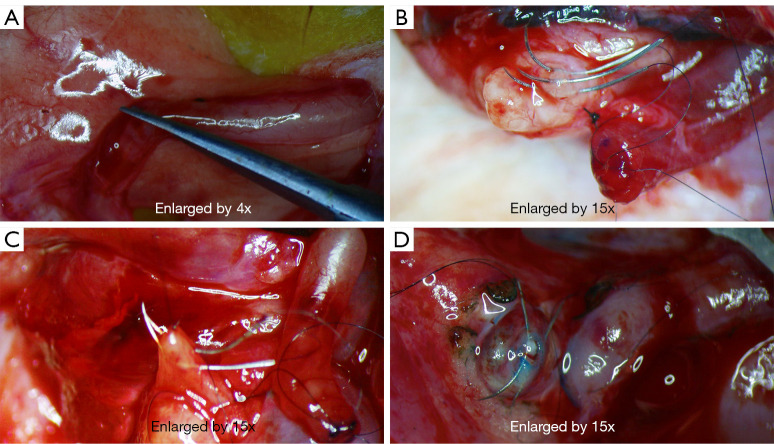
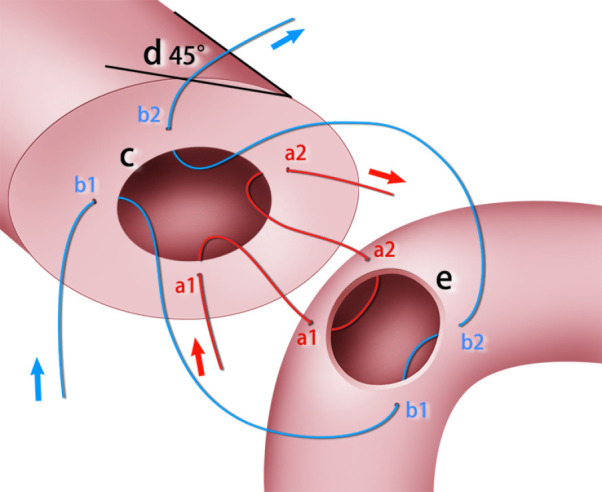
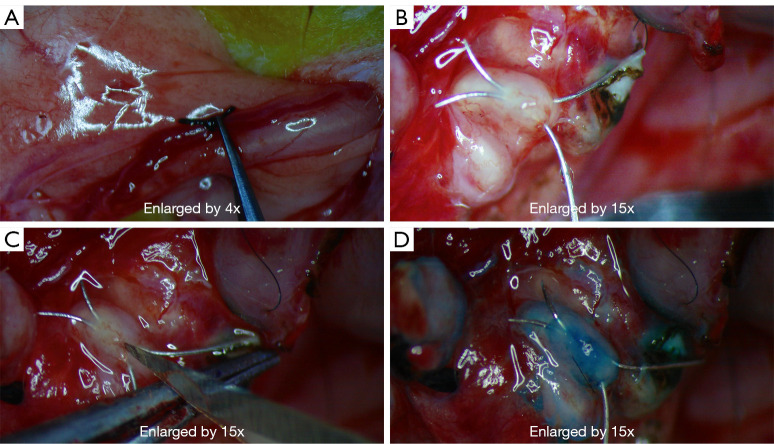
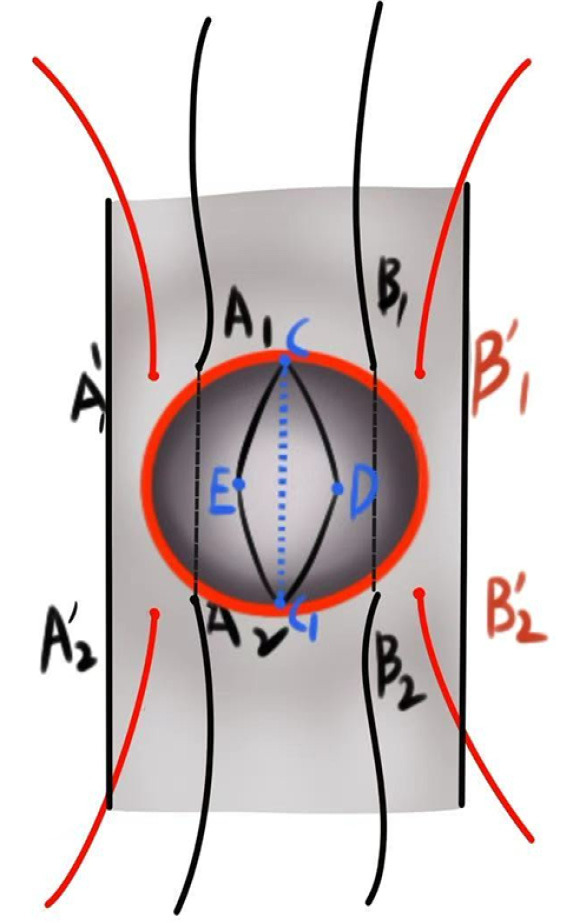
Methods: Thirty-three male rats (type: Sprague-Dawley, SD) were randomly divided into control (group I) and experimental groups (groups II and III). After 3 weeks of epididymal obstruction, bilateral vasoepididymostomy was performed. In group II, the epididymal tubules (the epididymal tubules, which were cut into circular incisions) were punctured and lifted with a suture under a microscope, the vas deferens was incised obliquely at 45° for CIVE. In group III: LIVE was performed. After 3 months, patency was assessed in a blinded manner.
Results: The rates of functional patency (presence of motile sperm in the vas deferens) were 90.9% and 63.6% in groups II and III, respectively (single-tailed test, P=0.042). On retrograde methylene blue vasography of the epididymis, the mechanical patency rate was similar to the functional patency rate. The incidence of sperm granulomas in postoperative groups II and III was 0% and 18.2%, respectively, with a single-tailed test P value of 0.24. Due to insufficient sample size, the sample size can be expanded for further verification in the later stage.
Conclusions: Compared with LIVE, CIVE at a 45° oblique incision of the vas deferens provides a larger anastomotic area and has a higher recanalization rate, which is worthy of further investigation. The aim of this study is to propose a new surgical approach called 'CIVE'. By expanding the anastomotic area to reduce the risk of traditional surgical failure, the ultimate goal is to provide patients with safer and more efficient treatment options.
Keywords: Microscopic vasoepididymostomy; epididymis; microsurgery; obstructive azoospermia (OA).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tau.amegroups.com/article/view/10.21037/tau-2025-91/coif). Q.T. receives consulting fees from the Key R&D projects in Lvliang City (No. 2022SHFZ12) and Research Project of Shanxi Provincial Health Commission (No. 2024222). The other authors have no conflicts of interest to declare.
Figures

References
-
- Practice Committee of the American Society for Reproductive Medicine in collaboration with the Society for Male Reproduction and Urology . Electronic address: asrm@asrm. The management of obstructive azoospermia: a committee opinion. Fertil Steril 2019;111:873-80. 10.1016/j.fertnstert.2019.02.013 - DOI - PubMed
LinkOut - more resources
Full Text Sources