

A case report of X-linked hypophosphatemia combined with primary hyperparathyroidism
- PMID: 40801029
- PMCID: PMC12339324
- DOI: 10.3389/fendo.2025.1634377
A case report of X-linked hypophosphatemia combined with primary hyperparathyroidism
Abstract
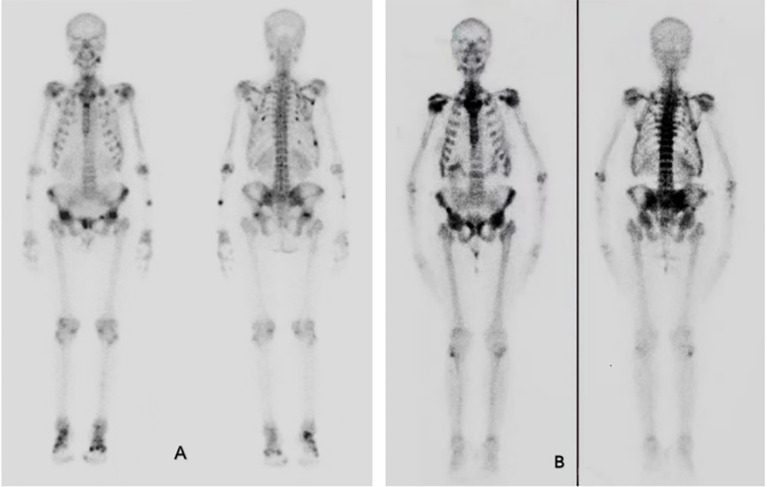
Both hypophosphatemic osteomalacia and primary hyperparathyroidism (PHPT) can lead to hypophosphatemia, but their simultaneous occurrence in the same patient is exceedingly rare. This article reports a case of a 43-year-old female patient whose primary clinical manifestations included pain in the lumbosacral and scapular regions, restricted mobility, and biochemical findings of decreased serum phosphate levels with normal parathyroid hormone (PTH) levels. The patient's symptoms improved after treatment with active vitamin D supplementation, although neutral phosphate supplements were not administered. Eight years later, the patient's symptoms progressively worsened. Further investigations revealed elevated PTH levels and worsening hypophosphatemia. Neck contrast-enhanced ultrasonography and parathyroid radionuclide imaging both indicated nodules in the right parathyroid gland. Postoperative pathological examination confirmed the diagnosis of parathyroid adenoma. Whole-exome sequencing identified a heterozygous deletion in exon 11 of the PHEX gene, consistent with a diagnosis of X-linked hypophosphatemia (XLH).
Keywords: X-linked hypophosphatemia; bone pain; hypophosphatemic osteomalacia; parathyroidectomy; primary hyperparathyroidism.
Copyright © 2025 Wu, Yang, Zhang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
X-Linked Hypophosphatemia.2012 Feb 9 [updated 2023 Dec 14]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2012 Feb 9 [updated 2023 Dec 14]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 22319799 Free Books & Documents. Review.
-
Real-world effectiveness of burosumab vs oral phosphate and active vitamin D in adults with X-linked hypophosphatemia.J Bone Miner Res. 2025 Jul 28;40(8):973-986. doi: 10.1093/jbmr/zjaf063. J Bone Miner Res. 2025. PMID: 40314226 Free PMC article.
-
An exceptionally rare case of a giant parathyroid adenoma with carcinoma-like presentation.Hormones (Athens). 2025 Jun;24(2):575-580. doi: 10.1007/s42000-025-00627-5. Epub 2025 Jan 20. Hormones (Athens). 2025. PMID: 39831932 Free PMC article.
-
Familial cases with adult-onset FGF23-related hypophosphatemic osteomalacia -A PHEX 3'-UTR change as a possible cause.Bone. 2024 May;182:117057. doi: 10.1016/j.bone.2024.117057. Epub 2024 Feb 25. Bone. 2024. PMID: 38412893
-
Parathyroidectomy for adults with primary hyperparathyroidism.Cochrane Database Syst Rev. 2023 Mar 8;3(3):CD013035. doi: 10.1002/14651858.CD013035.pub2. Cochrane Database Syst Rev. 2023. PMID: 36883976 Free PMC article.
References
-
- Xu C, Zhao J, Xia W. Guidelines for diagnosis and treatment of hypophosphatemic rickets/osteomalacia in China. Chin J Osteoporosis Bone Mineral Salt Dis. (2022) 15:107–25. doi: 10.3969/j.issn.1674-2591.2022.02.001 - DOI
-
- Guidelines for diagnosis and treatment of primary hyperparathyroidism. Chin J Osteoporosis Bone Mineral Salt Dis. (2014) 7:187–98. doi: 10.3969/j.issn.1674-2591.2014.03.002 - DOI
Publication types
LinkOut - more resources
Full Text Sources