

Granulocyte-Macrophage Colony-Stimulating Factor Inhibition Ameliorates Innate Immune Cell Activation, Inflammation, and Salt-Sensitive Hypertension
- PMID: 40801577
- PMCID: PMC12345731
- DOI: 10.3390/cells14151144
Granulocyte-Macrophage Colony-Stimulating Factor Inhibition Ameliorates Innate Immune Cell Activation, Inflammation, and Salt-Sensitive Hypertension
Abstract
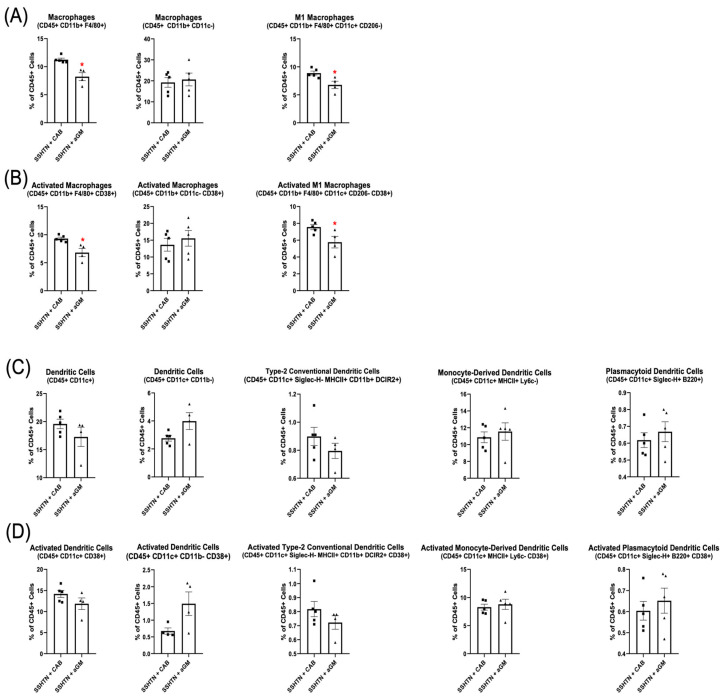
Hypertension (HTN) is a major contributor to global morbidity and manifests in several variants, including salt-sensitive hypertension (SSHTN). SSHTN is defined by an increase in blood pressure (BP) in response to high dietary salt, and is associated with heightened cardiovascular risk, renal damage, and immune system activation. However, the role of granulocyte-macrophage colony-stimulating factor (GM-CSF) has not yet been explored in the context of SSHTN. Previously, we reported that GM-CSF is critical in priming bone marrow-derived (BMD)-macrophages (BMD-Macs) and BMD-dendritic cells (BMD-DCs) to become activated (CD38+) in response to salt. Further exploration revealed these cells differentiated into BMD-M1 Macs, CD38+ BMD-M1 Macs, BMD-type-2 conventional DCs (cDC2s), and CD38+ BMD-cDC2s. Additionally, BMD-monocytes (BMDMs) grown with GM-CSF and injected into SSHTN mice traffic to the kidneys and differentiate into Macs, CD38+ Macs, DCs, and CD38+ DCs. In the current study, we treated SSHTN mice with an anti-GM-CSF antibody (aGM) and found that preventive aGM treatment mitigated BP, prevented renal inflammation, and altered renal immune cells. In mice with established SSHTN, aGM treatment attenuated BP, reduced renal inflammation, and differentially affected renal immune cells. Adoptive transfer of aGM-treated BMDMs into SSHTN mice resulted in decreased renal trafficking. Additionally, aGM treatment of BMD-Macs, CD38+ BMD-M1 Macs, BMD-DCs, and CD38+ BMD-cDC2s led to decreased pro-inflammatory gene expression. These findings suggest that GM-CSF plays a role in SSHTN and may serve as a potential therapeutic target.
Keywords: CD38; granulocyte-macrophage colony-stimulating factor; m1 macrophages; salt-sensitive hypertension; type 2-conventional dendritic cells.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






References
-
- Elijovich F., Weinberger M.H., Anderson C.A., Appel L.J., Bursztyn M., Cook N.R., Dart R.A., Newton-Cheh C.H., Sacks F.M., Laffer C.L., et al. Salt Sensitivity of Blood Pressure: A Scientific Statement From the American Heart Association. Hypertension. 2016;68:e7–e46. doi: 10.1161/HYP.0000000000000047. - DOI - PubMed
-
- Martin S.S., Aday A.W., Almarzooq Z.I., Anderson C.A.M., Arora P., Avery C.L., Baker-Smith C.M., Barone Gibbs B., Beaton A.Z., Boehme A.K., et al. 2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association. Circulation. 2024;149:e347–e913. doi: 10.1161/CIR.0000000000001209. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
