

Association between long-term (current) aspirin use and sepsis-related delirium in elderly patients: a retrospective cohort study
- PMID: 40802113
- PMCID: PMC12350516
- DOI: 10.1007/s40520-025-03152-y
Association between long-term (current) aspirin use and sepsis-related delirium in elderly patients: a retrospective cohort study
Abstract
Background: Driven by the global aging trend, the prognosis of elderly patients with sepsis has garnered increasing attention. Sepsis-associated delirium (SAD), a common manifestation of elderly patients with sepsis, is frequently linked to poor clinical outcomes. Despite its prevalence, effective preventive measures remain lacking. Pharmacological interventions have emerged as promising components of a comprehensive strategy for the treatment and prevention of delirium. Among them, aspirin-renowned for its anti-inflammatory properties, affordability, and safety-may hold particular promise, given the central role of inflammation in the pathogenesis of both sepsis and delirium. Early initiation of anti-inflammatory therapy may offer a more effective approach to preventing SAD and enhancing patient outcomes.
Aims: To investigate the association between long-term (current) aspirin use and the incidence of SAD in elderly septic patients.
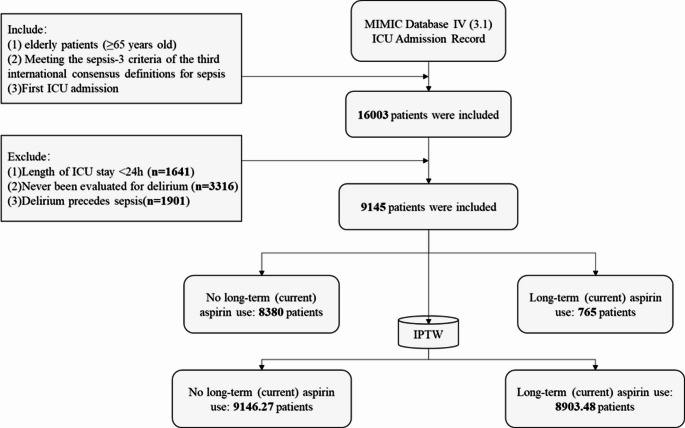
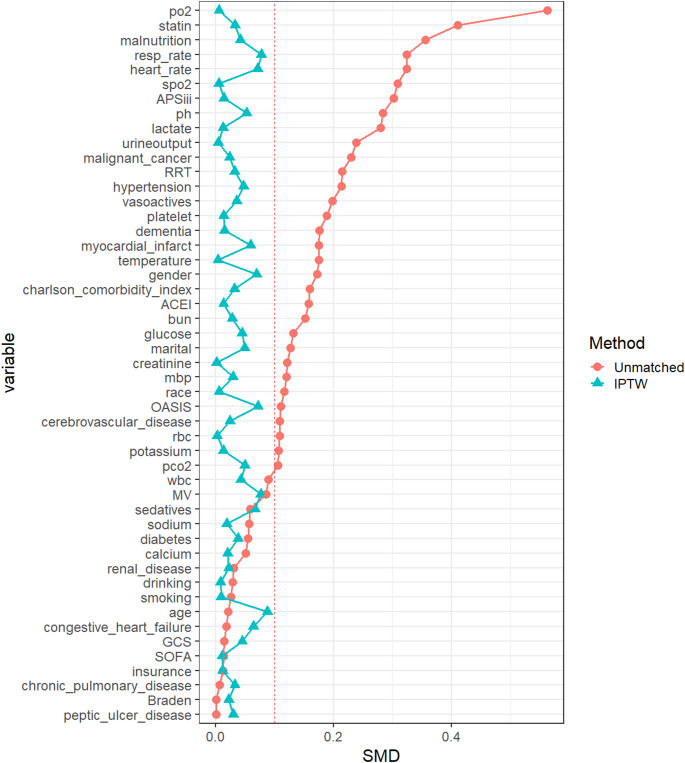
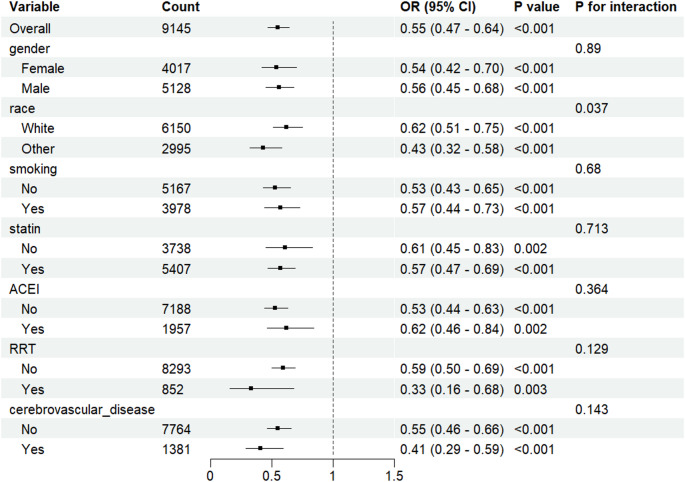
Methods: We extracted and analyzed data from 9145 elderly septic patients. The primary outcome, SAD, was analyzed using multivariable logistic regression to explore the correlation between long-term (current) aspirin use and the incidence of SAD. To ensure the robustness of the results, inverse probability of treatment weighting was used to adjust Intergroup relations. Finally, subgroup analyses were conducted.
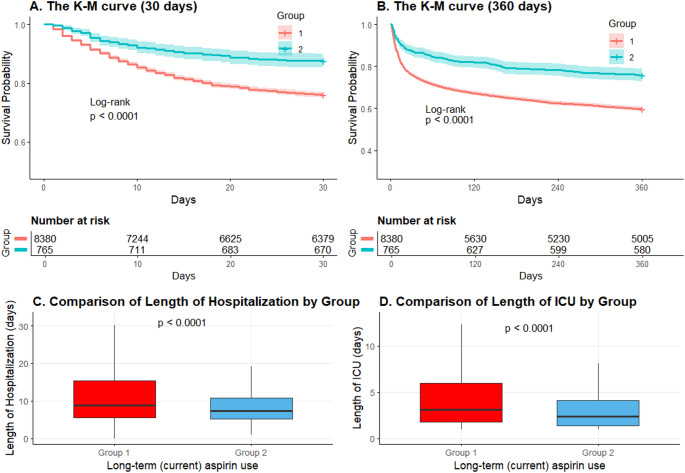
Results: 765 elderly septic patients were long-term (current) aspirin users, with a SAD incidence rate of 31.9% (244/765). In contrast, 8380 elderly septic patients without a history of long-term (current) aspirin use had a SAD incidence rate of 46.1% (3863/8380). After adjusting for 49 covariates, the multivariable logistic regression results showed that long-term (current) aspirin use was negatively associated with the risk of SAD (adjusted OR: 0.78, p < 0.001). Even after balancing group differences through inverse probability treatment weighting, the results remained stable.
Conclusions: In elderly patients, long-term (current) aspirin use is negatively associated with the incidence of SAD and is also linked to improved clinical outcomes.
Keywords: Delirium; Long-term (current) use of aspirin; NSAIDs; Neuropsychological tests; Older people; Sepsis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: The Medical Information Mart for Intensive Care IV (MIMIC-IV) database was supported by grants from the National Institute of Biomedical Imaging and Bioengineering (NIBIB) of the National Institutes of Health (NIH) under award numbers R01-EB001659 (2003–2013) and R01-EB017205 (2014–2018) and approved by the Institutional Review Boards of Beth Israel Deaconess Medical Center (Boston, MA) and the Massachusetts Institute of Technology (Cambridge, MA). Patient consent statement: Data extracted from the MIMIC-IV database do not require individual informed consent because the research data is publicly available, and all patient data are de-identified. Competing interests: The authors declare no competing interests.
Figures
References
-
- Kotfis K, Wittebole X, Jaschinski U et al (2019) A worldwide perspective of sepsis epidemiology and survival according to age: observational data from the ICON audit. J Crit Care 51:122–132. 10.1016/j.jcrc.2019.02.015 - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J et al (2001) Epidemiology of severe sepsis in the united states: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:1303–1310. 10.1097/00003246-200107000-00002 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
