

Mutational analysis of primary and advanced chordoma tissue using next-generation sequencing
- PMID: 40802536
- PMCID: PMC12348310
- DOI: 10.1002/cncr.70033
Mutational analysis of primary and advanced chordoma tissue using next-generation sequencing
Abstract
Background: Chordomas are rare ectodermal bone malignancies derived from transformed notochordal remnants. Histologic variants include conventional (80%-90%), chondroid (5%-15%), and dedifferentiated (2%-8%). Because chordomas are relatively resistant to chemotherapy and radiotherapy, novel targeted agents are needed to expand treatment approaches and improve outcomes. This study analyzes the genomic landscape of chordoma and identifies potential pathogenic and druggable targets.
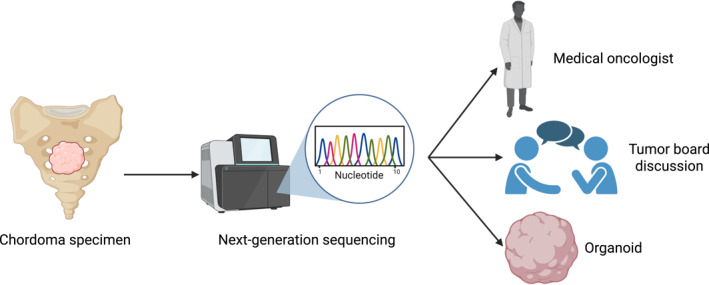
Methods: Eighty-six tumor samples derived from chordoma patients treated at Massachusetts General Hospital, University of California, Los Angeles, and the University of Miami were included. Tumor specimens were sent for comprehensive molecular profiling using next-generation sequencing. The most frequently mutated genes were identified and categorized by subtype, and microsatellite instability and programmed death ligand-1 (PD-L1) staining were assessed.
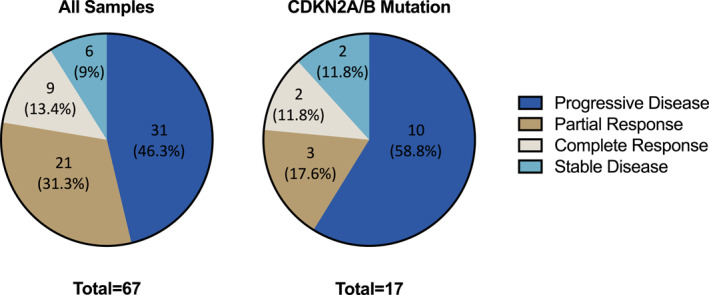
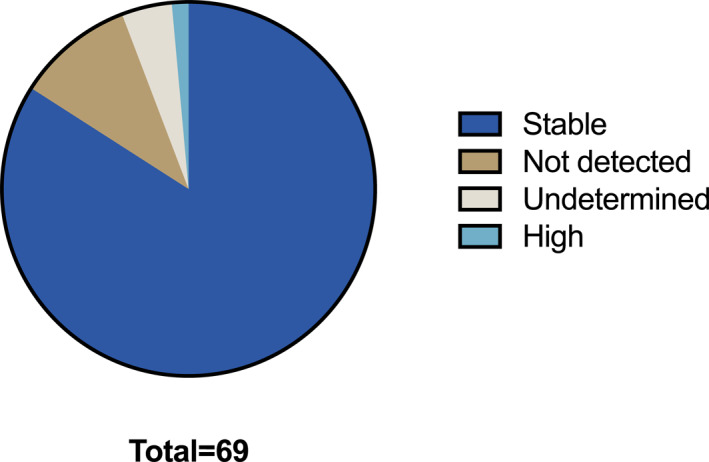
Results: Histologic subtypes included 70 conventional (81.4%), nine chondroid (10.5%), and seven dedifferentiated chordomas (8.1%). The most common mutations were cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B) (28 of 86, 33%), low-density lipoprotein receptor-related protein 1B (10 of 86, 12%), polybromo-1 (9 of 86, 11%), and epidermal growth factor receptor (EGFR) (8 of 86, 9%). By subtype, CDKN2A/B mutation was most common in conventional chordoma (24 of 70, 34%), and chondroid chordoma (3 of 9, 33%). CDKN2A/B and EGFR mutations were most common in dedifferentiated chordoma (2/7, 29%). Microsatellite instability was not detected in seven of 69 (10.1%) samples. PD-L1 staining of tumor and immune cells was scarce, with scores <1 in 38 of 41 (92.7%) and 22 of 25 (88%) patients, respectively.
Conclusions: This study provides a robust, high-dimensional sequencing assessment from 86 chordoma tissue samples and a descriptive overview of the genomic landscape of this rare, difficult to treat malignancy. Future studies should include in vitro assessment of gain and loss of function of frequently altered pathways to validate these findings.
Keywords: CDKN2A/B; PD‐L1; chordoma; molecular profiling; mutational analysis; next‐generation sequencing.
© 2025 The Author(s). Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
Brooke Crawford reports consulting fees from Zimmer Biomet Holdings, Inc; and fees for professional activities from IlluminOss Medical, Inc. Elizabeth L. Lord reports consulting fees from Globus Medical, Inc and SI‐BONE, Inc. Arun Singh reports consulting fees from Deciphera Pharmaceuticals Inc. The other authors declare no conflicts of interest.
Figures
Similar articles
-
Can a Liquid Biopsy Detect Circulating Tumor DNA With Low-passage Whole-genome Sequencing in Patients With a Sarcoma? A Pilot Evaluation.Clin Orthop Relat Res. 2025 Jan 1;483(1):39-48. doi: 10.1097/CORR.0000000000003161. Epub 2024 Jun 21. Clin Orthop Relat Res. 2025. PMID: 38905450
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
-
Unraveling molecular advancements in chordoma tumorigenesis and treatment response: a review of scientific discoveries and clinical implications.Neurosurg Focus. 2024 May;56(5):E18. doi: 10.3171/2024.2.FOCUS2417. Neurosurg Focus. 2024. PMID: 38691860 Review.
-
Targeted therapy for advanced anaplastic lymphoma kinase (<I>ALK</I>)-rearranged non-small cell lung cancer.Cochrane Database Syst Rev. 2022 Jan 7;1(1):CD013453. doi: 10.1002/14651858.CD013453.pub2. Cochrane Database Syst Rev. 2022. PMID: 34994987 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
