

EHRA perspective on the digital data revolution in arrhythmia management: insights from the association's annual summit
- PMID: 40802569
- PMCID: PMC12345632
- DOI: 10.1093/europace/euaf149
EHRA perspective on the digital data revolution in arrhythmia management: insights from the association's annual summit
Abstract
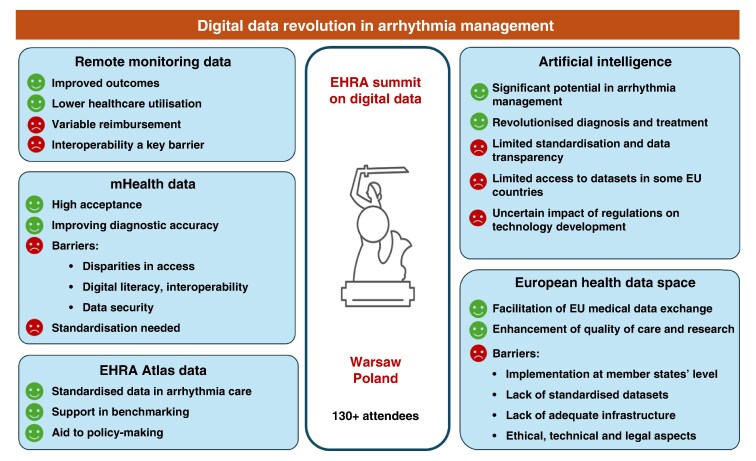
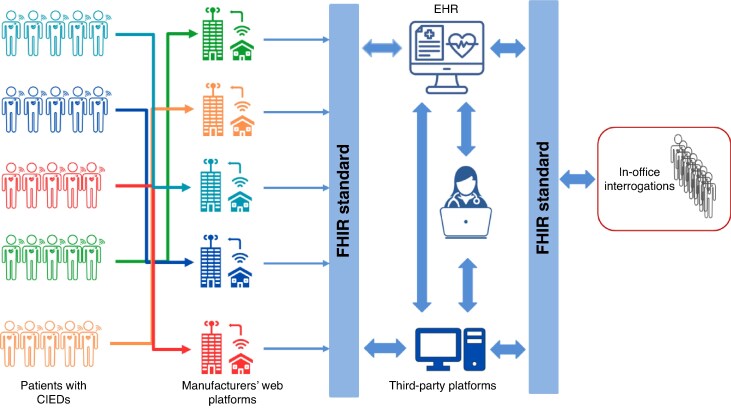
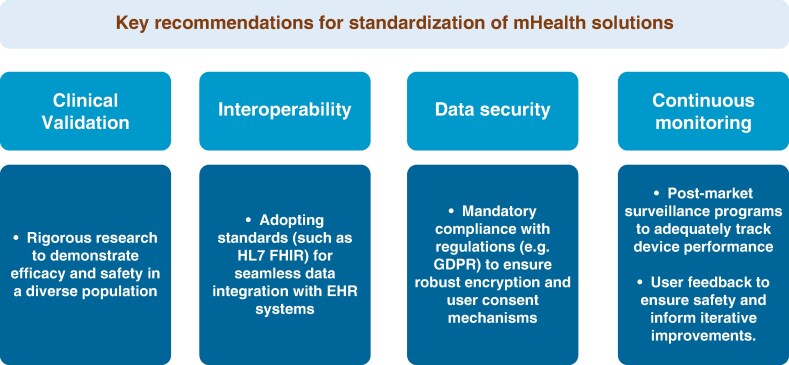
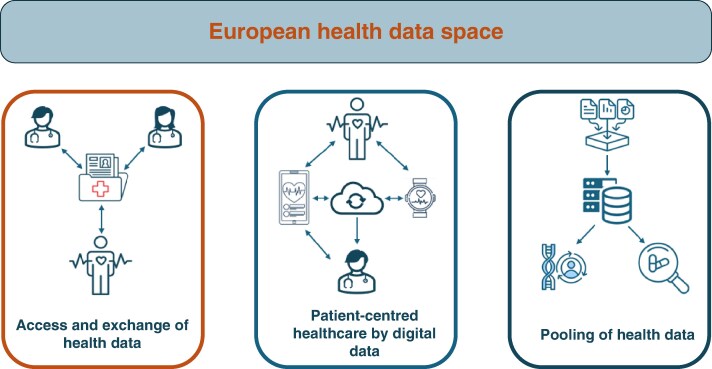
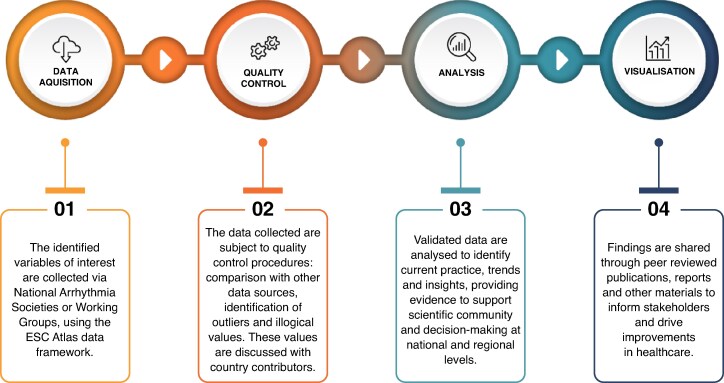
The 2024 European Heart Rhythm Association (EHRA) Summit in Warsaw focused on the digital transformation of arrhythmia management, convening over 130 stakeholders from academia, industry, and policy. This review summarises the current state (in 2025) and future directions of digital health in arrhythmia care, including remote monitoring (RM) of cardiac implantable electronic devices (CIEDs), mobile health (mHealth), artificial intelligence (AI), and integration into the European Health Data Space (EHDS). RM has become central to CIED follow-up, improving outcomes and reducing healthcare use. However, challenges in reimbursement, workforce adaptation, and data interoperability persist. The absence of standardised data exchange between device vendors and healthcare systems has led to initiatives like the World Forum on CIED follow-up to develop interoperability standards. mHealth tools, including apps and wearable devices, offer accurate arrhythmia detection but face regulatory, digital literacy, and privacy barriers. The EHDS aims to enable cross-border data sharing for personalised care and real-world research, though implementation must address ethical, legal, and infrastructural issues. AI shows promise in prediction, monitoring, and data integration, but lacks standardised, transparent validation. The ESC-EHRA Atlas in Heart Rhythm Disorders supports structured data collection to harmonize and benchmark care across Europe. Overall, digital innovations, if coupled with regulatory alignment, interoperability standards, and equitable access, have the potential to shift arrhythmia management toward a more predictive, personalized, and efficient model of care.
Keywords: Arrhythmia; Artificial intelligence; CIEDs; Digital health; EHRA; European Health Data Space; Health data integration; Interoperability; Remote monitoring; mHealth.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: C.L.F. reports receiving compensation for teaching and proctoring from Medtronic and Biotronik SE & Co. D.D. received modest lecture honoraria, travel grants and/or a fellowship grant from Abbott, Astra Zeneca, Biotronik, Boehringer Ingelheim, Boston Scientific, Bristol Myers Squibb, CVRx, Daiichi Sankyo, Medtronic, Microport, Pfizer, Sanofi, ZOLL. E.A. reports speaker fees for Medtronic, Biosense Webster and Bristol-Myers-Squibb; Consulting for Boston Scientific. G.B. reports speaker's fees of small amount from Bayer, Boston, BMS, Daiichi-Sankyo, Janssen, Sanofi. G.L.B. reports speaker's fees (small amount) from Abbott, Boston Scientific, Biotronik, Medtronic, MIcroport, Bayer Heathcare, Daiichi Sankyo; Pfizer. H.H. received personal lecture and consultancy fees from, Biotronik, Daiichi-Sankyo, Downtown Europe, IZIDOK, European Society of Cardiology, and Viatris Pharmaceuticals Inc. He received unconditional research grants through the University of Antwerp and/or the University of Hasselt from Abbott, Bayer, Boehringer-Ingelheim, Biosense-Webster, Boston-Scientific, Daicchi-Sankyo, Viatris Pharmaceuticals Inc, Novo Nordisk, Novartis, and Pfizer-BMS, all outside the scope of this work. H.B. has received institutional research and fellowship support, speaker fees, travel grants, and/or advisory boards from Abbott, Biotronik, Boston Scientific, Medtronic Microport. H.P. received speaker´s honoraria and consultancy fees from Abbott, Boston Scientific, Biotronik, Medtronic, Johnson and Johnson Medtech. J.LM. has received fees and honoraria for lectures, education and scientific advice from Abbott, Biotronik, Daiichi-Sankyo, Everpace, Johnson&Johnson, Zio & Zoll. M.M.F. received consultancy/speaker fees from Abbott, Biosense-Webster, Medtronic, Pfizer. P.S. reports receiving speakers’ honoraria from Boehringer Ingelheim, Novartis, AstraZeneca, Samsung Medison, GE Ultrasound. R.C.-A. reports receiving speaker’s honoraria of small amount from Abbott and Boston Scientific. V.T. reports receiving speakers’ honoraria or travel grants from: Boehringer Ingelheim, Novartis, Pfizer, Servier, J&J, Astra Zeneca, Medtronic. Proctorship fees: Abbott, Biotronik. S.B. is a consultant for Medtronic, Boston Scientific, Microport, and Zoll. D.S., K.M.-R., N.D. and R.H. do not report any disclosures.
Figures

References
-
- Akar JG, Bao H, Jones PW, Wang Y, Varosy PD, Masoudi FA et al. Use of remote monitoring is associated with lower risk of adverse outcomes among patients with implanted cardiac defibrillators. Circ Arrhythm Electrophysiol 2015;8:1173–80. - PubMed
-
- Saxon LA, Hayes DL, Gilliam FR, Heidenreich PA, Day J, Seth M et al. Long-term outcome after ICD and CRT implantation and influence of remote device follow-up: the ALTITUDE survival study. Circulation 2010;122:2359–67. - PubMed
-
- Varma N, Piccini JP, Snell J, Fischer A, Dalal N, Mittal S. The relationship between level of adherence to automatic wireless remote monitoring and survival in pacemaker and defibrillator patients. J Am Coll Cardiol 2015;65:2601–10. - PubMed
-
- Hindricks G, Taborsky M, Glikson M, Heinrich U, Schumacher B, Katz A et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet 2014;384:583–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
