

SCORE: Serologic evidence of COVID-19 and social and occupational contacts in healthcare workers in long-term care and acute care facilities in Southeastern Ontario (SCORE)
- PMID: 40802698
- PMCID: PMC12349196
- DOI: 10.1371/journal.pone.0303813
SCORE: Serologic evidence of COVID-19 and social and occupational contacts in healthcare workers in long-term care and acute care facilities in Southeastern Ontario (SCORE)
Abstract
Introduction: We established a longitudinal cohort of healthcare workers (HCWs) in an acute care hospital (ACH) and four long-term care homes (LTCHs) in Ontario, Canada, to follow the incidence of SARS-CoV-2 infection, humoral immune response to infection and/or vaccination, and determinants of infection risk. Here, we 1) describe the cohort regarding the distribution of main exposures, outcomes and serologic assays, 2) describe the unadjusted incidence of SARS-CoV-2 infection risk in the overall population, and 3) summarize the analysis and its pertinence.
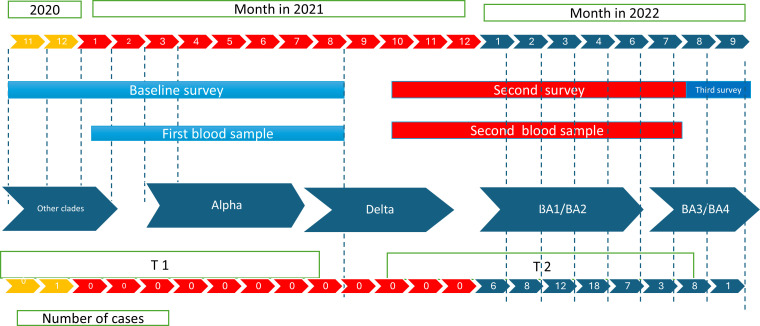
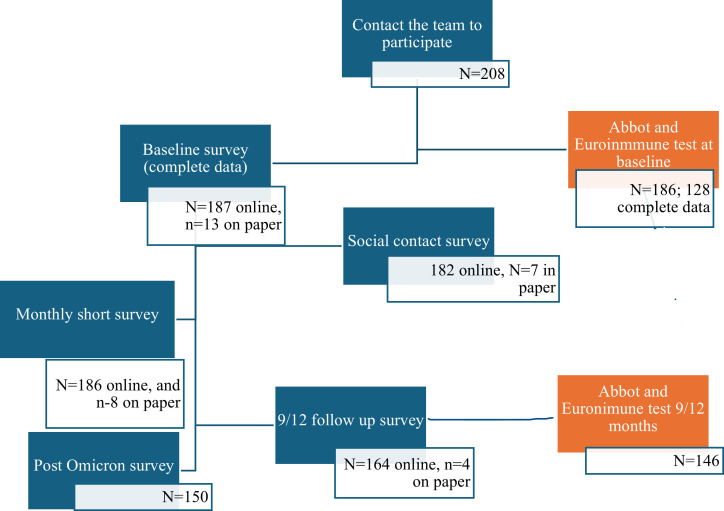
Methods and participants: HCWs were recruited between November 24, 2020, and July 24, 2021. They completed a baseline survey, monthly surveillance for 9-12 months, a post-Omicron-wave survey, and provided blood samples for anti-SARS-CoV-2 antibody measurements. We collected data on host-related (humoral response to vaccines and SARS-CoV-2 infection) and environmental factors (social contact history and occupational, household and community conditions). Descriptive analysis by setting, comparison of distributions, and unadjusted survival analysis were performed.
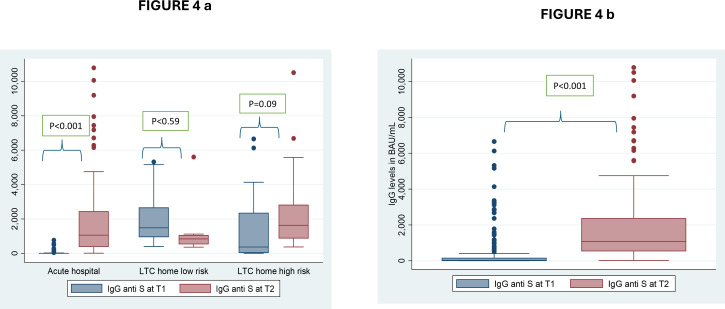
Results: In total, 143 HCWs from the ACH and 57 from LTCHs had complete data, and 72% were followed until September 2022. Nearly 60% of the sample consisted of nurses, nurse assistants and personal support workers. Survival analysis showed that the risk of infection was bimodal, with low risk throughout the study period until the first Omicron wave. ACH HCWs had a higher risk of infection during the Omicron waves than during the preceding waves (Odds Ratio = 7.64; CI95%: 4.24-13.7), while LTCH HCWs at high-risk facilities experienced a similar risk of infection before and during the Omicron waves (OR = 1.76; CI95%: 0.63-4.9). During the Omicron waves, the use of protective equipment by HCWs working with institutional COVID-19 cases increased, but the use of community protective measures diminished. Household infections reported by participating HCWs also increased during the Omicron waves compared to previous waves. Immunoglobulin G (IgG) antibody levels increased over two time periods, (Pre vs Post- Omicron) likely due to the immune response to high levels of both vaccination and SARS-CoV-2 infections.
Discussion: We observed a low incidence of COVID-19 until the onset of the Omicron waves, which highlights the drastic impact of this Variants of Concern (VOC) on transmission and the importance of infectious agent characteristics. Our analysis indicated a ninefold increased risk of infection compared to that in earlier pandemic periods. Further analysis will allow the estimation of 1) the risk factors for SARS-CoV-2 infection at the community, household and healthcare facility levels, 2) the relationship between humoral responses and SARS-CoV-2 infection/vaccination, and 3) the role of social contact in work, household and community settings in the risk of infection.
Copyright: © 2025 Martinez-Cajas et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Antibody tests for identification of current and past infection with SARS-CoV-2.Cochrane Database Syst Rev. 2022 Nov 17;11(11):CD013652. doi: 10.1002/14651858.CD013652.pub2. Cochrane Database Syst Rev. 2022. PMID: 36394900 Free PMC article.
-
Anti-SARS-CoV-2 Antibody Levels in a Cohort of Health Care Workers Before and After the Omicron Wave in Canada.J Assoc Med Microbiol Infect Dis Can. 2025 May 29;10(2):127-145. doi: 10.3138/jammi-2024-0029. eCollection 2025 Jun. J Assoc Med Microbiol Infect Dis Can. 2025. PMID: 40673053 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article.
-
The effect of sample site and collection procedure on identification of SARS-CoV-2 infection.Cochrane Database Syst Rev. 2024 Dec 16;12(12):CD014780. doi: 10.1002/14651858.CD014780. Cochrane Database Syst Rev. 2024. PMID: 39679851 Free PMC article.
References
-
- Canada PHA of. COVID-19 infections among people working in healthcare settings. 2021. [cited 2024 March 20]. Available from: https://www.canada.ca/en/public-health/services/diseases/coronavirus-dis...
-
- CIHI. Canadian Institute for Health Information. COVID-19 Cases and Deaths in Health Care Workers in Canada — Data Tables. Ottawa, ON: CIHI; March 31, 2022.
-
- Carazo S, Laliberté D, Villeneuve J, Martin R, Deshaies P, Denis G, et al. Characterization and evolution of infection control practices among severe acute respiratory coronavirus virus 2 (SARS-CoV-2)-infected healthcare workers in acute-care hospitals and long-term care facilities in Québec, Canada, Spring 2020. Infect Control Hosp Epidemiol. 2022;43(4):481–9. doi: 10.1017/ice.2021.160 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
