

Single-cell RNA sequencing identifies the prolactin receptor as a therapeutic target in adenomyosis
- PMID: 40804233
- PMCID: PMC12350698
- DOI: 10.1038/s41392-025-02339-z
Single-cell RNA sequencing identifies the prolactin receptor as a therapeutic target in adenomyosis
Abstract
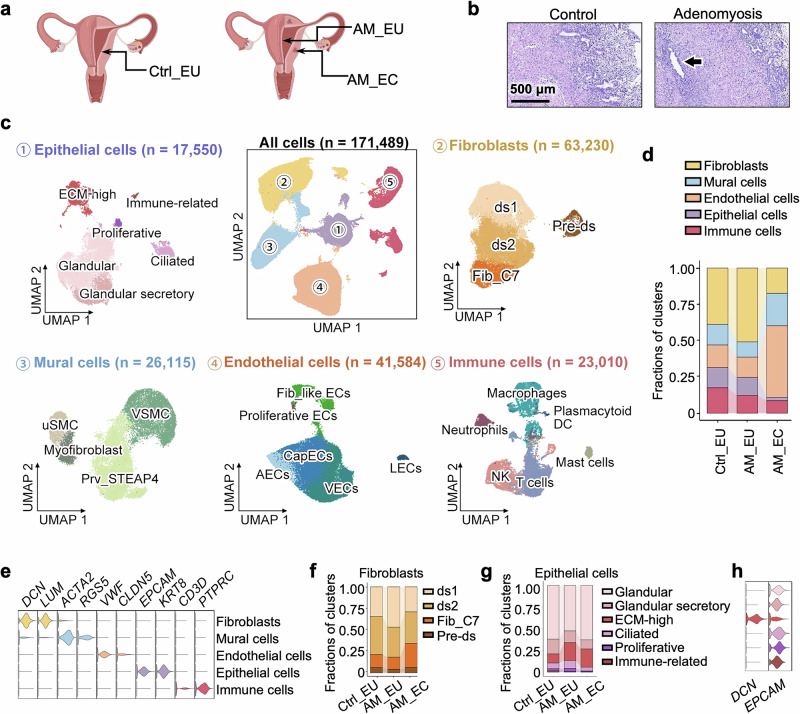
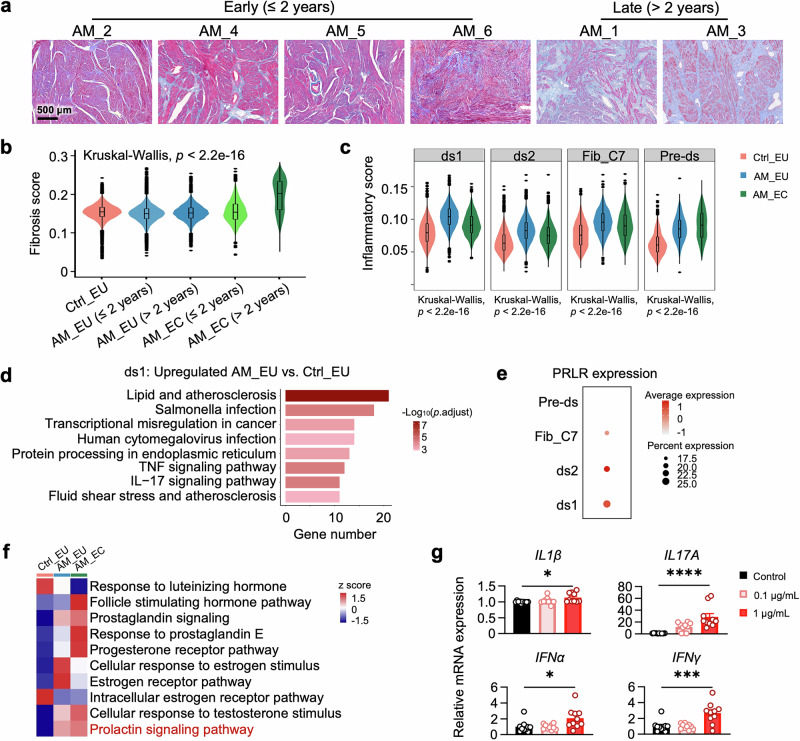
Adenomyosis is a complex gynecological disease characterized by endometrial tissue invasion into the myometrium. Current interventions, such as hormonal therapy or hysterectomy, are associated with significant side effects and compromise fertility, underscoring the urgent need for safe and effective treatments. Using single-cell RNA sequencing (scRNA-seq) of uterine samples from patients, we identified prolactin (PRL) signaling as a key pathological driver of adenomyosis. Specifically, scRNA-seq revealed a distinct epithelial subcluster with enriched PRL receptor (PRLR) expression. PRL signaling is overactivated in this epithelial subcluster, promoting cellular survival and proliferation, which contributes to lesion formation and expansion in adenomyosis. Concurrently, PRLR is also highly expressed in a fibroblast subcluster characterized by strong expression of inflammation-related genes. Pathological PRL hyperactivation was further validated in preclinical animal models, where transgenic overexpression of PRL or pituitary transplantation induced an adenomyosis phenotype. Importantly, we demonstrated that dysregulation of local PRL signaling led to the development and progression of adenomyosis, whereas inhibition of PRLR with the monoclonal antibody HMI-115 markedly ameliorated pathological manifestations. These findings establish PRL signaling as a critical driver of adenomyosis pathogenesis, highlighting PRLR inhibition as a promising therapeutic strategy and demonstrating the translational potential of HMI-115 for treating adenomyosis, a gynecological condition that has long been neglected in drug development.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures



References
-
- Bird, C. C., McElin, T. W. & Manalo-Estrella, P. The elusive adenomyosis of the uterus-revisited. Am. Jobstet. Gynecol.112, 583–593 (1972). - PubMed
-
- Gordts, S., Grimbizis, G. & Campo, R. Symptoms and classification of uterine adenomyosis, including the place of hysteroscopy in diagnosis. Fertil. Steril.109, 380–388.e381 (2018). - PubMed
-
- Levgur, M., Abadi, M. A. & Tucker, A. Adenomyosis: symptoms, histology, and pregnancy terminations. Obstet. Gynecol.95, 688–691 (2000). - PubMed
-
- Chapron, C. et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum. Reprod. Update26, 392–411 (2020). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
