

Factors associated with cryptococcal capsular antigen positivity among people living with HIV: a retrospective observational cohort study
- PMID: 40804366
- PMCID: PMC12344822
- DOI: 10.1186/s12879-025-11417-0
Factors associated with cryptococcal capsular antigen positivity among people living with HIV: a retrospective observational cohort study
Abstract
Background: Cryptococcosis, which is caused by Cryptococcus, is an aggressive fungal disease posing a high mortality risk among people living with HIV (PLHIV). However, factors associated with cryptococcal capsular antigen (CrAg) positivity among PLHIV remain unclear.
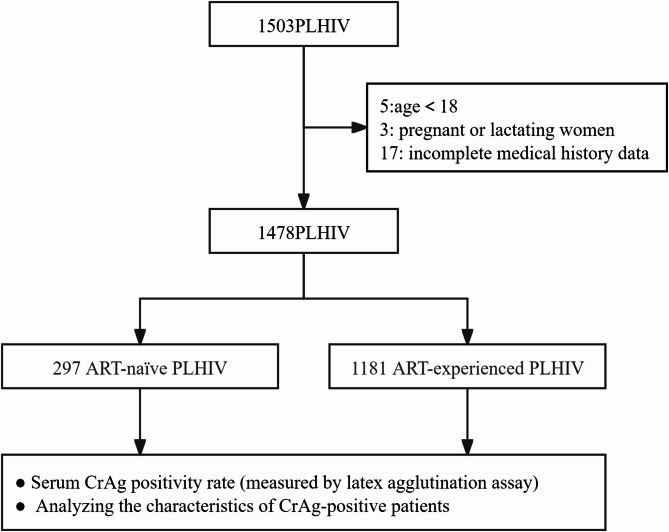
Methods: We recruited PLHIV from the Guangzhou Eighth People's Hospital between March 2018 and December 2019. Serum CrAg was qualitatively detected using Lateral Flow Assay. Fungal culture and pathological examinations were performed on cerebrospinal fluid. Chi-squared tests and multivariable logistic regression were used to identify factors associated with CrAg positivity.
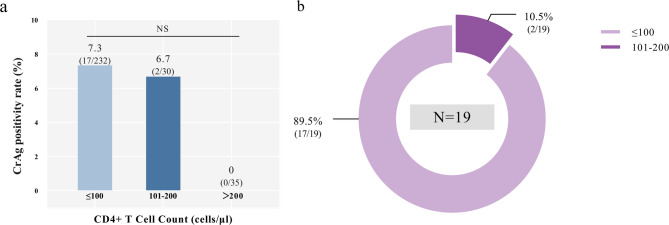
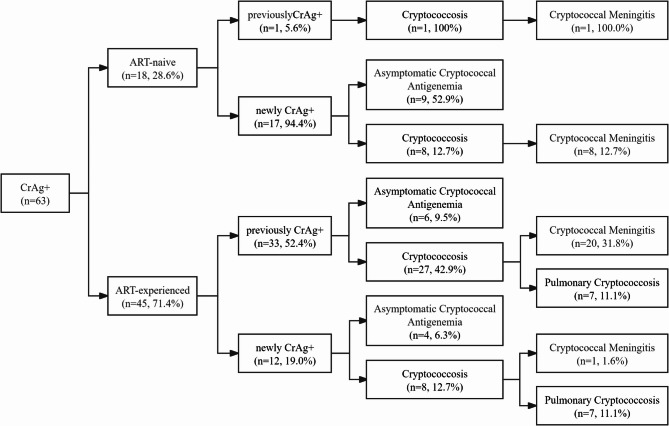
Results: A total of 1478 PLHIV were included, among whom 297 (20.1%) were antiretroviral therapy-naïve (ART-naïve), 1181 (79.9%) were ART-experienced. The median baseline CD4 + T cell count was 43 cells/μl (interquartile range [IQR]:13-117). The overall CrAg positivity rate was 5.1%, with 94.7% of CrAg-positive individuals having baseline CD4 + counts ≤ 200 cells/μl. CrAg positivity was 6.4% among ART-naïve and 4.7% among ART-experienced PLHIV. Notably, within the ART-experienced group, CrAg-positive PLHIV displayed lower baseline and latest CD4 + T cell counts than those in CrAg-negative PLHIV. CrAg status was significantly associated with shorter ART duration (≤ 1 year vs. > 2 year: adjusted odds ratio [aOR], 2.53; 95% confidence interval [CI], 1.20-5.34. 1-2 year vs. > 2 year: 4.61, 2.10-10.12) and other OIs (2.56, 1.41-4.63) among ART-experienced PLHIV.
Conclusions: A considerable CrAg positivity rate was observed among both ART-naïve and ART-experienced PLHIV. CD4 + T cell count ≤ 200 cells/μl, shorter ART duration, and presence of other opportunistic infections were all significantly associated with CrAg positivity. These findings support extending serum CrAg screening to all PLHIV with CD4 + counts ≤ 200 cells/μl, regardless of ART status, to improve early detection and reduce cryptococcosis-related mortality.
Keywords: ART; CrAg; PLHIV; Positivity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the institutional review board of the Guangzhou Eighth People’s Hospital (Approval number: 202034167). Informed consent was signed by all participants at enrollment. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures



References
-
- Hagen F, Khayhan K, Theelen B, Kolecka A, Polacheck I, Sionov E, et al. Recognition of seven species in the Cryptococcus gattii/Cryptococcus neoformans species complex. Fungal Genet Biol. 2015;1(78):16–48. - PubMed
-
- Gullo FP, Rossi SA, Sardi JDCO, Teodoro VLI, Mendes-Giannini MJS, Fusco-Almeida AM. Cryptococcosis: epidemiology, fungal resistance, and new alternatives for treatment. Eur J Clin Microbiol Infect Dis. 2013;32(11):1377–91. - PubMed
-
- Park BJ, Wannemuehler KA, Marston BJ, Govender N, Pappas PG, Chiller TM. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23(4):525. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
