

Efficacy comparison between dentofacial orthopedic treatment and adenotonsillectomy on children with obstructive sleep apnea and skeletal class II malocclusion: a retrospective study
- PMID: 40804385
- PMCID: PMC12351886
- DOI: 10.1186/s12903-025-06697-6
Efficacy comparison between dentofacial orthopedic treatment and adenotonsillectomy on children with obstructive sleep apnea and skeletal class II malocclusion: a retrospective study
Abstract
Objective: This study aims to evaluate the effects of dentofacial orthopedic treatment (DOT) and adenotonsillectomy (AT) in Obstructive Sleep Apnea (OSA) children with skeletal Class II malocclusion and adenotonsillar hypertrophy (ATH), focusing on changes in sleep respiratory function, anatomic and aerodynamic characteristics of upper airway (UA).
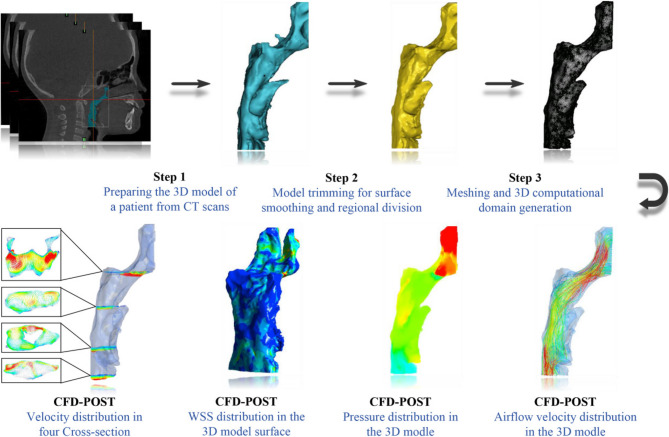
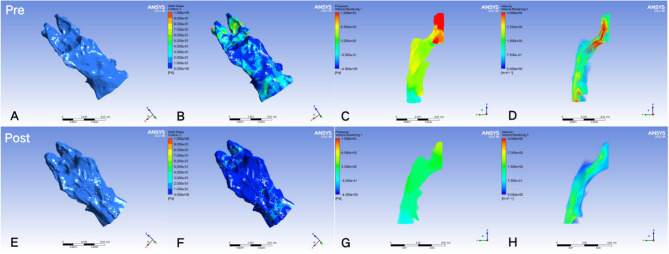
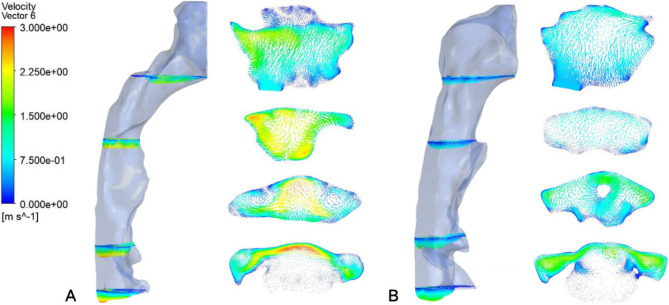
Methods: In this retrospective study, 38 OSA children (mean age: 8.42 years, 15 females and 23 males) were included consecutively. Patients were categorized into two groups: DOT group (n = 20) and AT group (n = 18). Baseline (T0) and follow-up (T1) assessments involved polysomnography and radiological examinations to evaluate improvements in sleep quality as well as changes in craniofacial morphology and UA variables. Aerodynamic parameters such as airflow velocity, airway resistance, and wall shear stress were quantified using computational fluid dynamics.
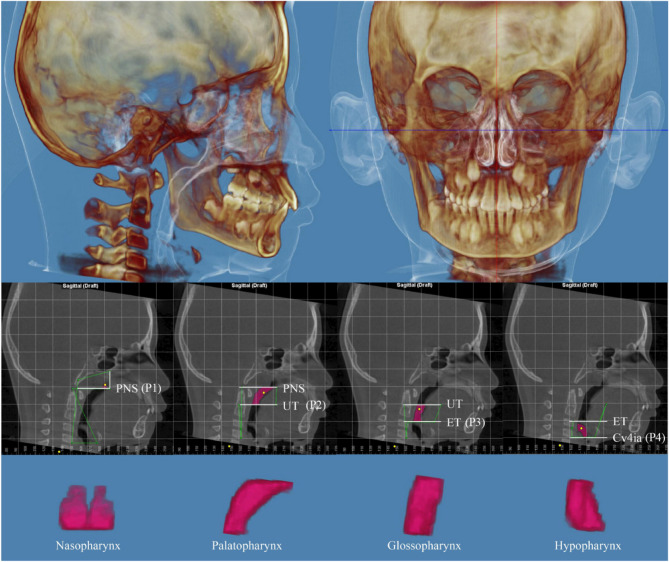
Results: In the comparative analysis of sleep respiratory functions, there were no significant differences in apnea-hypopnea index changes between the treatment groups (DOT group: -3.72/h, AT group: -3.32/h, P = 0.600). In the DOT group, UA's volume average enlargements were observed in the nasopharynx, palatopharynx, glossopharynx, and hypopharynx by 54.5%, 41.6%, 34.0%, and 22.5%, respectively. In comparison, the AT group showed enlargements of 66.0%, 20.1%, 62.9%, and - 1.0%, respectively. In terms of UA aerodynamic characteristics, there were no significant differences between two groups.
Conclusions: In OSA children with skeletal Class II malocclusion and ATH, DOT as a non-invasive approach, has shown improvements in respiratory function comparable to AT, as evidenced by changes in the UA's anatomical and aerodynamic characteristics.
Keywords: Adenotonsillectomy; Children; Computational fluid dynamics; Dentofacial orthopedic treatment; OSA; Skeletal class II malocclusion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This retrospective study was approved by the Research Ethics Committee of Shanghai Stomatological Hospital (approval no. 2023/012). All patients and their parents signed informed consent and authorizing the use of the examinations for research purposes. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Trial registration: This study was registered with the Chinese Clinical Trial Registry (ChiCTR), registration number ChiCTR2500102383.
Figures



References
-
- Gottlieb D, Punjabi N. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–400. - PubMed
-
- Lo Bue A, Salvaggio A, Insalaco G. Obstructive sleep apnea in developmental age. A narrative review. Eur J Pediatrics. 2020;179(3):357–65. - PubMed
-
- Marcus C, Brooks L, Draper K, Gozal D, Halbower A, Jones J, et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2012;130(3):e714–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
