

Peripheral cytokine and monocyte phenotype associations in drug-resistant epilepsy
- PMID: 40804444
- PMCID: PMC12350764
- DOI: 10.1038/s41598-025-14402-4
Peripheral cytokine and monocyte phenotype associations in drug-resistant epilepsy
Abstract
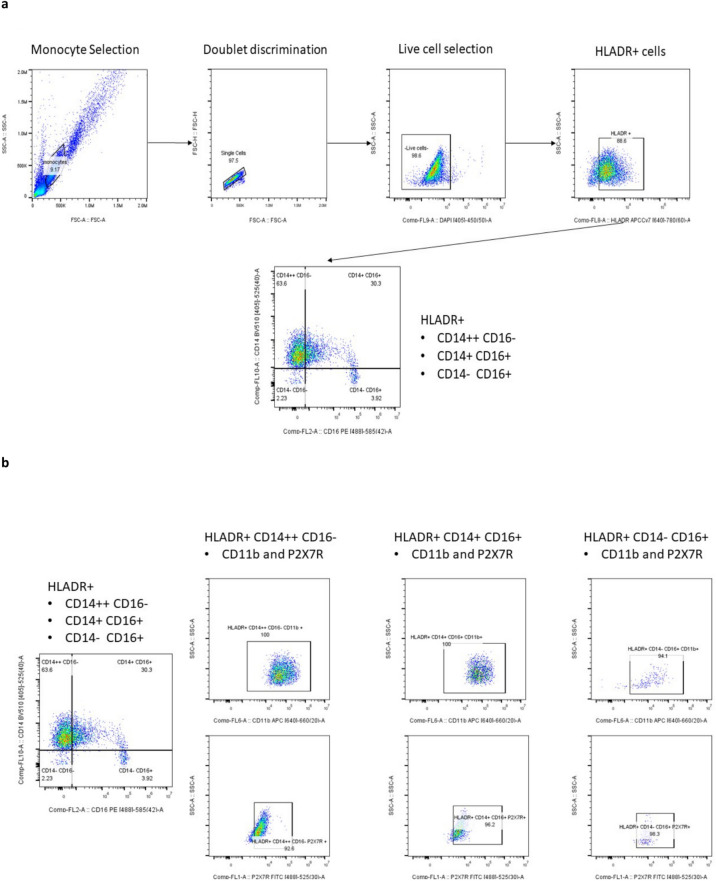
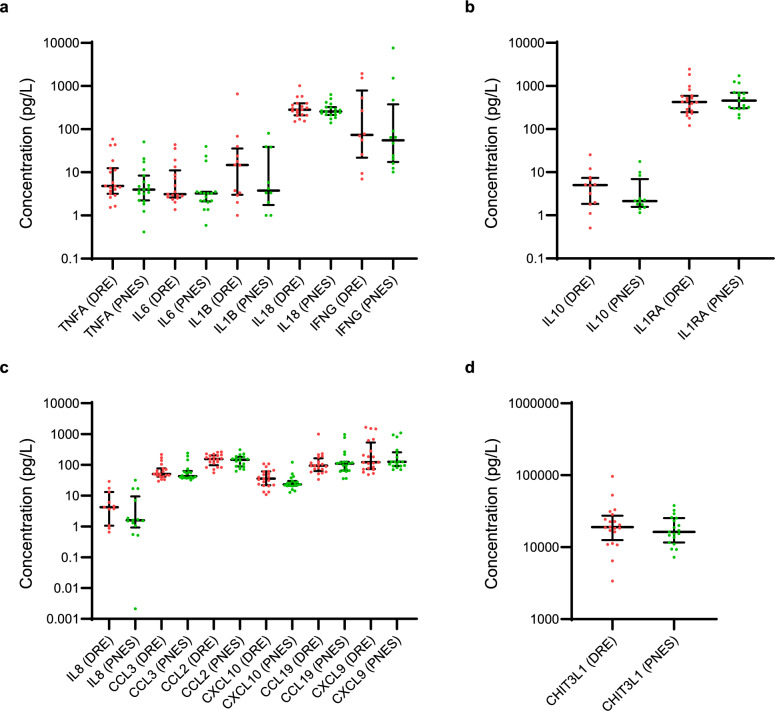
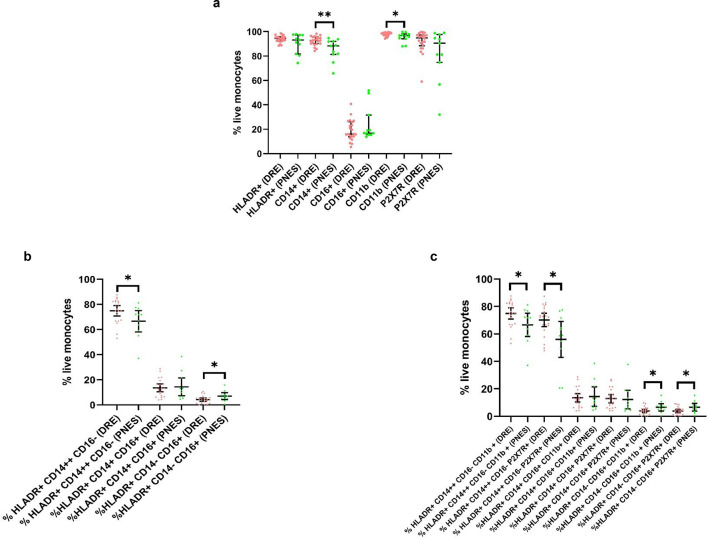
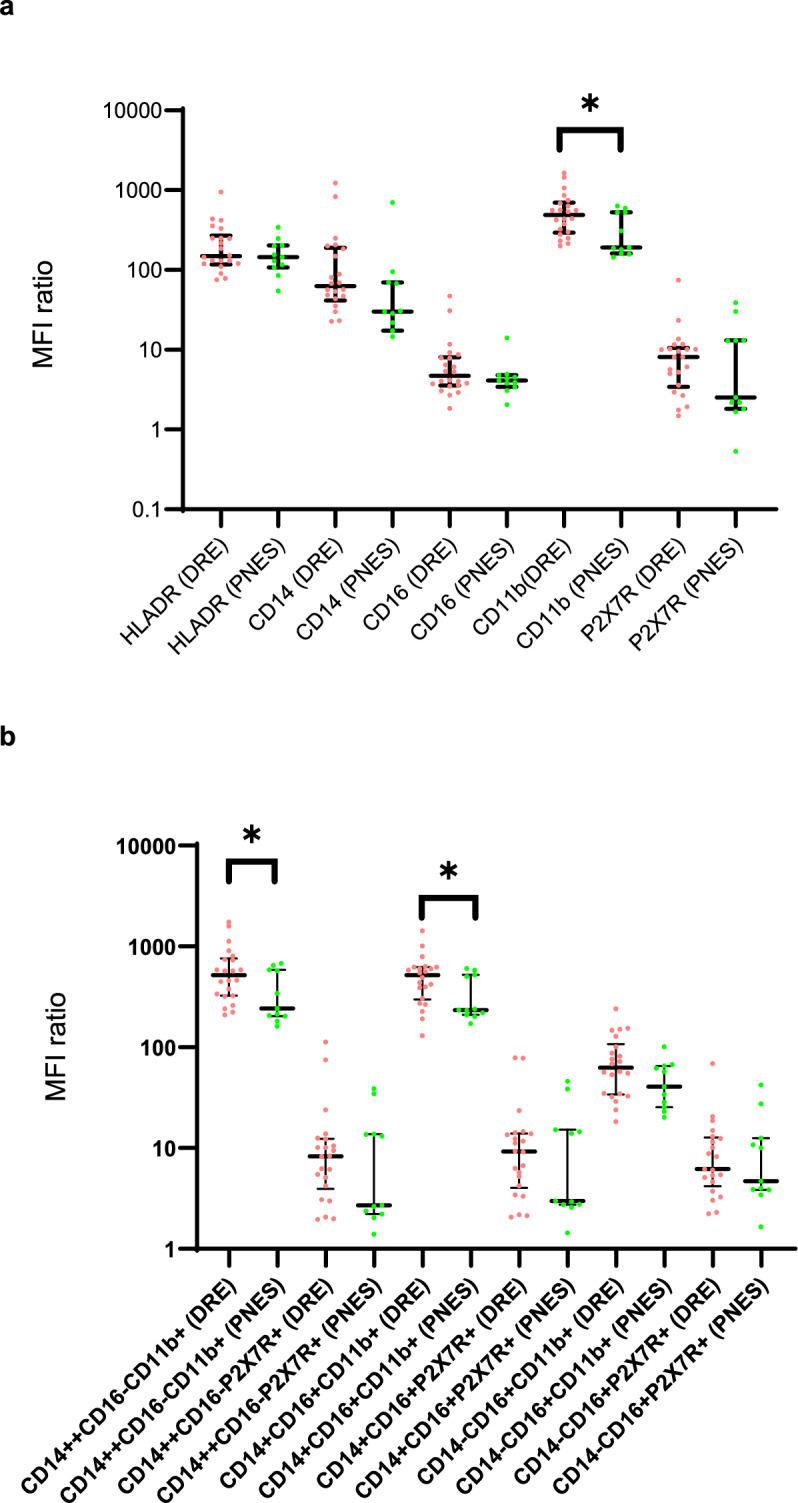
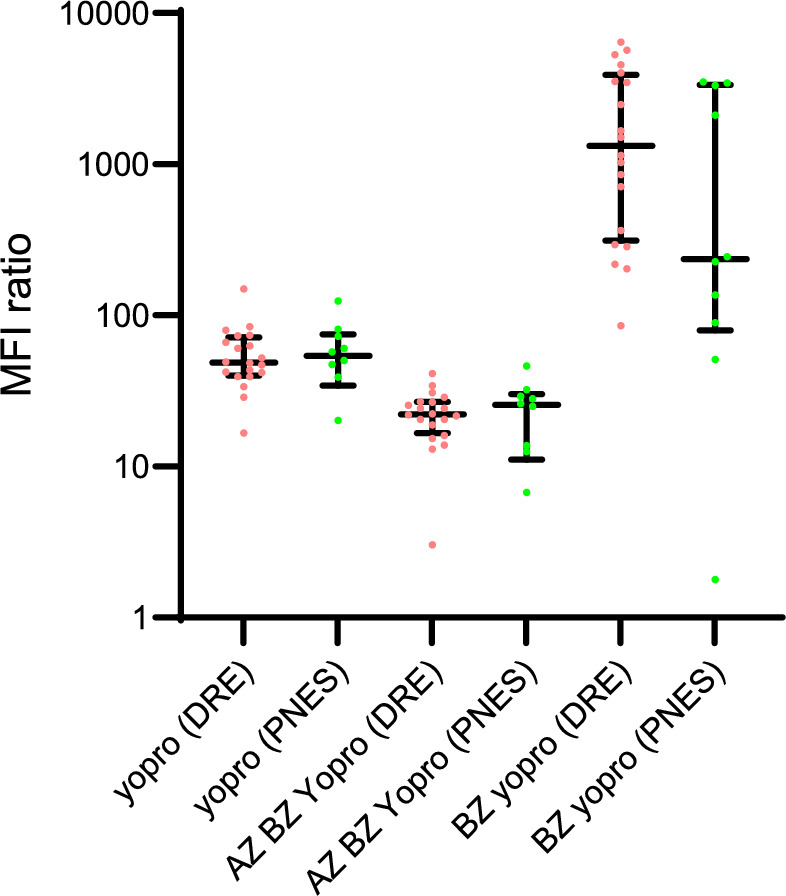
Novel therapeutic targets are required to develop new treatments to lower the rates of drug-resistant epilepsy (DRE). This study assessed differences in plasma inflammatory biomarker concentrations and monocyte phenotype and function in patients with DRE versus psychogenic non-epileptic seizures (PNES). Luminex was used to analyse plasma samples from 21 DRE cases and 19 PNES controls for concentrations of selected cytokines and chitinase 3-like 1 (CHI3L1). Flow cytometry was used to quantify the percentage of monocytes expressing HLADR, CD14, CD16, CD11b, P2X7R and their median fluorescence intensity (MFI) ratio in 22 DRE and 11 PNES patients. Flow cytometry was used to assess P2X7 receptor (P2X7R) pore function via YO-PRO-1 uptake. No difference in cytokine and CHI3L1 concentrations was seen. Compared to PNES, DRE had a higher percentage of 'classical' monocytes (CD14++CD16-) and less 'non-classical' monocytes (CD14-CD16+). The percentage of 'classical' monocytes expressing P2X7R was increased in DRE compared to PNES. CD11b MFI ratio was increased in 'classical' and 'intermediate' (CD14+CD16+) monocytes. P2X7R pore function was similar between groups. Overall, while cytokine levels were similar between groups, the differences in monocyte phenotype indicates a more 'proinflammatory' circulating innate immune state in DRE. Thus, monocytes may be a novel therapeutic target for future research.
Keywords: Chitinase 3-like 1; Cytokine; Drug resistant epilepsy; Monocyte; P2X7 receptor; Psychogenic non-epileptic seizures.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: TT was supported by an Australian Government Research Training Program (RTP) Scholarship. She has received travel support from Biogen. PP is supported by an Emerging Leadership 2 Investigator Grant from the NHMRC (APP2017651), The University of Melbourne and Monash University, and receives research grant funding from the NHMRC and MRFF. He has received speaker honoraria or consultancy fees to his institution from Chiesi, Eisai, LivaNova, Sun Pharma, Supernus, The Limbic, and UCB Pharma, outside the submitted work. He is Deputy Editor for Epilepsia Open. PK is supported by a NHMRC Investigator Grant (GNT2025849). He and/or his institution has received research support or consultancy fees from Angelini, Eisai, Jazz Pharmaceuticals, LivaNova, SK Life Science and UCB Pharma. TJO is supported by a NHMRC Investigator Grant (APP1176426), and has received grant research funding from the MRFF, ARC, NIH and DoD. His institution has received research funding for his research and consultancies from Chiesi, Eisai, Biogen, ES Therapeutics, Epidarex, LivaNova, Novartis, Supernus, and UCB Pharma, outside the submitted work. MM is supported by NHMRC MRFF grant (APP1201062) and NHMRC Ideas grant. She has received funding from Brain Foundation, Charles and Sylvia Viertel Foundation, Bethlehem Griffith Foundation and MS Research Australia. She has served on advisory board for Merck, Alexion, and has received speaker honoraria from Merck. Her institution receives Australian National Health Medical Research Council. The remaining authors have no conflicts of interest.
Figures
Similar articles
-
Psychogenic non-epileptic seizures in patients undergoing epilepsy surgery: experience from a tertiary referral center.Epilepsy Behav. 2025 Jul 15;171:110592. doi: 10.1016/j.yebeh.2025.110592. Online ahead of print. Epilepsy Behav. 2025. PMID: 40669171
-
Circulating monocytes upregulate CD52 and sustain innate immune function in cirrhosis unless acute decompensation emerges.J Hepatol. 2025 Jul;83(1):146-160. doi: 10.1016/j.jhep.2024.12.031. Epub 2025 Jan 14. J Hepatol. 2025. PMID: 39818234
-
A pilot study on the programming protocol of vagus nerve stimulation in children with drug-resistant epilepsy: High pulse amplitude or high duty cycle.Epilepsia Open. 2025 Jun;10(3):831-841. doi: 10.1002/epi4.70043. Epub 2025 Apr 22. Epilepsia Open. 2025. PMID: 40261679 Free PMC article. Clinical Trial.
-
Yoga for epilepsy.Cochrane Database Syst Rev. 2017 Oct 5;10(10):CD001524. doi: 10.1002/14651858.CD001524.pub3. Cochrane Database Syst Rev. 2017. PMID: 28982217 Free PMC article.
-
Systemic treatments for metastatic cutaneous melanoma.Cochrane Database Syst Rev. 2018 Feb 6;2(2):CD011123. doi: 10.1002/14651858.CD011123.pub2. Cochrane Database Syst Rev. 2018. PMID: 29405038 Free PMC article.
Cited by
-
Uniaxial compressive strength of cemented coal gangue backfill based on response surface methodology.Sci Rep. 2025 Aug 14;15(1):29837. doi: 10.1038/s41598-025-14635-3. Sci Rep. 2025. PMID: 40813875 Free PMC article.
References
-
- Ravizza, T. et al. Mtor and neuroinflammation in epilepsy: Implications for disease progression and treatment. Nat. Rev. Neurosci.25(5), 334–350 (2024). - PubMed
-
- Wesselingh, R. et al. Seizures in autoimmune encephalitis: Kindling the fire. Epilepsia61(6), 1033–1044 (2020). - PubMed
-
- Aronica, E. et al. Complement activation in experimental and human temporal lobe epilepsy. Neurobiol. Dis.26(3), 497–511 (2007). - PubMed
-
- Soltani Khaboushan, A., Yazdanpanah, N. & Rezaei, N. Neuroinflammation and proinflammatory cytokines in epileptogenesis. Mol. Neurobiol.59(3), 1724–1743 (2022). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
