

Trajectory-based analysis of early mechanical ventilation PEEP levels and physiological parameter trajectories in ARDS patients and their association with the occurrence of gastrointestinal injury events
- PMID: 40804672
- PMCID: PMC12351905
- DOI: 10.1186/s12890-025-03856-x
Trajectory-based analysis of early mechanical ventilation PEEP levels and physiological parameter trajectories in ARDS patients and their association with the occurrence of gastrointestinal injury events
Abstract
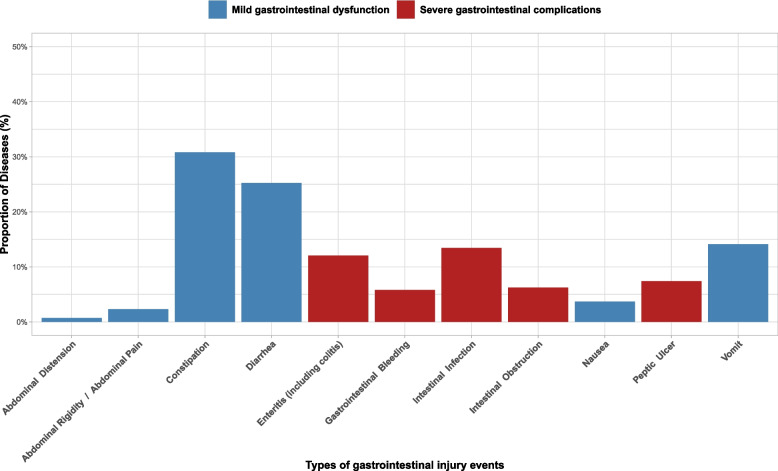
Background: Mechanical ventilation is crucial in the treatment of acute respiratory distress syndrome (ARDS), but is associated with complications, including gastrointestinal injury (GI). This study investigates the association between early mechanical ventilation parameter trajectories and the occurrence of GI events in ARDS patients.
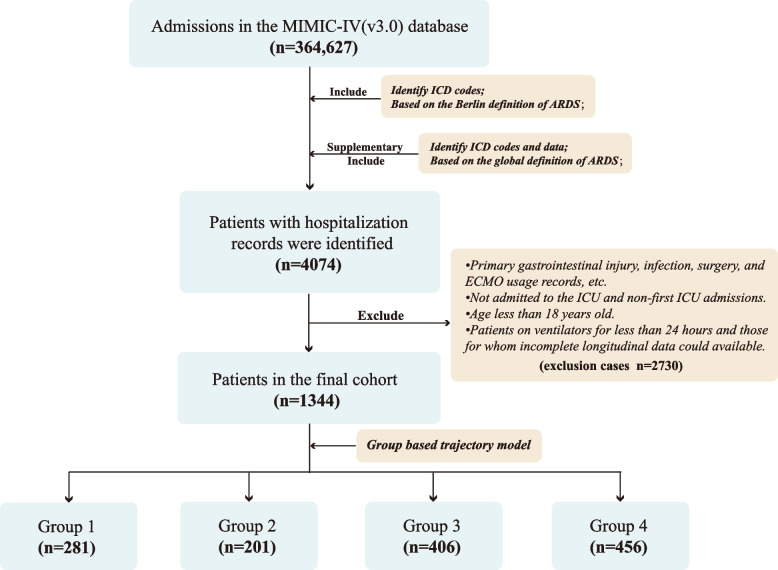
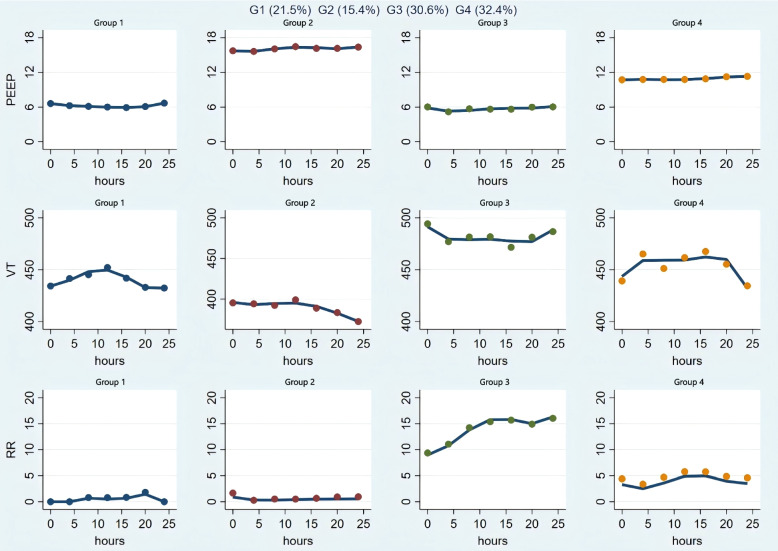
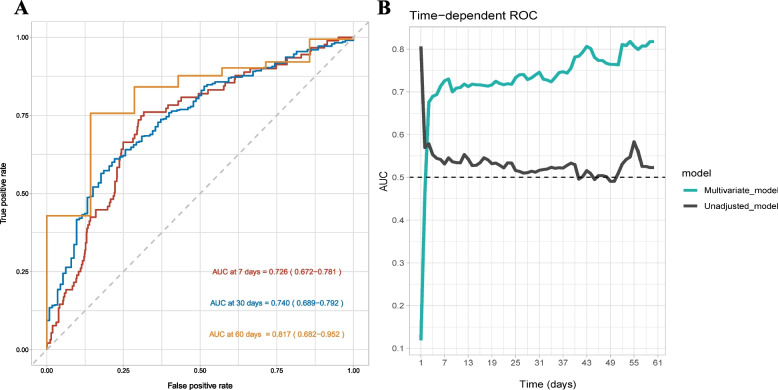
Methods: A retrospective cohort study using the MIMIC-IV database employed group-based trajectory modeling (GBTM) to identify trajectory patterns during early mechanical ventilation in ARDS patients. Kaplan-Meier analysis estimated GI events incidence across trajectory groups, and Cox regression models assessed independent risk associations, adjusting for clinical confounders. We evaluated and compared the model in order to enhance its robustness.
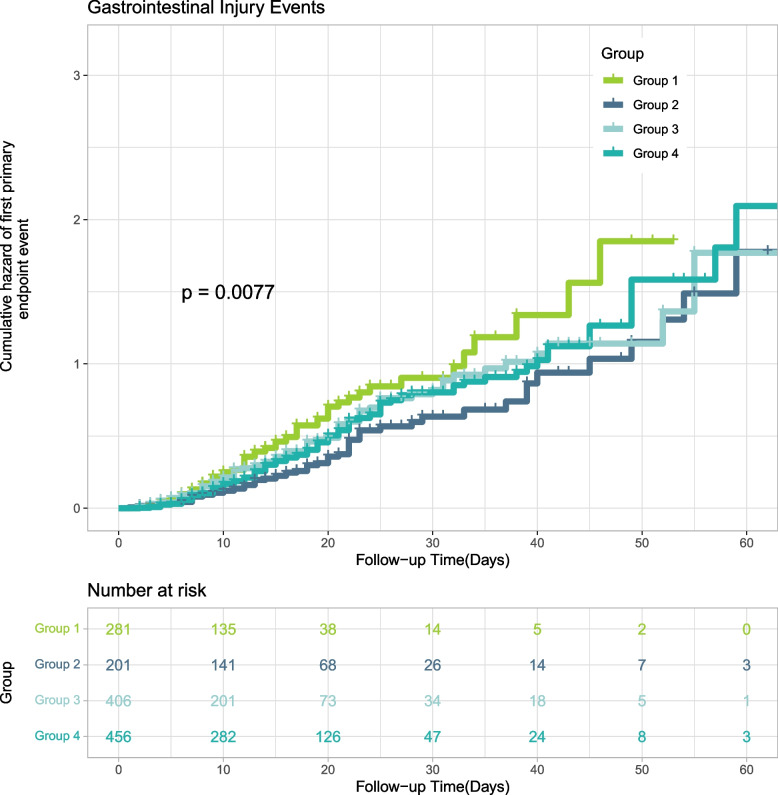
Results: A total of 1,344 ARDS patients were included, with four trajectory groups identified. Patients in Group 1 (low PEEP, moderate VT, lower frequency spontaneous breathing) exhibited the highest GI risk, while Group 2 (high PEEP, low tidal volume, controlled spontaneous breathing) had the lowest risk (HR: 0.606, 95% CI: 0.418-0.879, P = 0.008). Kaplan-Meier curves revealed a consistent pattern with Group 1 showing the highest cumulative incidence of GI events. Aspirin use, heparin therapy, renal replacement therapy, and APACHE II score were identified as independent factors for GI events. Subgroup analysis did not show intergroup differences. Sensitivity analyses confirmed model robustness.
Conclusions: Ventilation parameter trajectories are associated with GI injury risk in ARDS patients. Strategies optimizing PEEP levels and spontaneous breathing may mitigate this risk, supporting the need for individualized ventilation approaches.
Keywords: ARDS; Gastrointestinal injury; Group-based trajectory modeling; MIMICIV Database; Mechanical ventilation; PEEP.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The data used in this study were derived from the MIMICIV database, and database access was approved for sharing with informed consent amnesty by the Institutional Review Boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Centre. One of the authors (STH) passed the appropriate tests and was granted permission to extract the data (Permission ID: 58312537). Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Early spontaneous breathing for acute respiratory distress syndrome in individuals with COVID-19.Cochrane Database Syst Rev. 2022 Jun 29;6(6):CD015077. doi: 10.1002/14651858.CD015077. Cochrane Database Syst Rev. 2022. PMID: 35767435 Free PMC article.
-
Higher PEEP versus Lower PEEP Strategies for Patients with Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis.Ann Am Thorac Soc. 2017 Oct;14(Supplement_4):S297-S303. doi: 10.1513/AnnalsATS.201704-338OT. Ann Am Thorac Soc. 2017. PMID: 29043834
-
Positioning for acute respiratory distress in hospitalised infants and children.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD003645. doi: 10.1002/14651858.CD003645.pub4. Cochrane Database Syst Rev. 2022. PMID: 35661343 Free PMC article.
-
High versus low positive end-expiratory pressure (PEEP) levels for mechanically ventilated adult patients with acute lung injury and acute respiratory distress syndrome.Cochrane Database Syst Rev. 2013 Jun 6;2013(6):CD009098. doi: 10.1002/14651858.CD009098.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2021 Mar 30;3:CD009098. doi: 10.1002/14651858.CD009098.pub3. PMID: 23740697 Free PMC article. Updated.
-
Extracorporeal carbon dioxide removal for the treatment of acute hypoxaemic respiratory failure: the REST RCT.Health Technol Assess. 2025 Jul;29(33):1-16. doi: 10.3310/GJDM0320. Health Technol Assess. 2025 Jul;29(33):1-16. doi: 10.3310/GJDM0320. PMID: 40758387 Clinical Trial.
References
-
- Wick KD, Ware LB, Matthay MA. Acute respiratory distress syndrome. BMJ (Clinical research ed). 2024;387:e076612. 10.1136/bmj-2023-076612. - PubMed
-
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet (London, England). 1967;2(7511):319–23. 10.1016/s0140-6736(67)90168-7. - PubMed
-
- Slutsky AS. History of mechanical ventilation. From Vesalius to ventilator-induced lung injury. Am J Respir Crit Care Med. 2015;191(10):1106–15. 10.1164/rccm.201503-0421PP. - PubMed
-
- Putensen C, Wrigge H, Hering R. The effects of mechanical ventilation on the gut and abdomen. Curr Opin Crit Care. 2006;12(2):160–5. 10.1097/01.ccx.0000216585.54502.eb. - PubMed
-
- Reintam A, Parm P, Kitus R, Kern H, Starkopf J. Gastrointestinal symptoms in intensive care patients. Acta Anaesthesiol Scand. 2009;53(3):318–24. 10.1111/j.1399-6576.2008.01860.x. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
