

Clinical efficacy analysis of LNG-IUS tail anchoring to the superficial myometrium under hysteroscopic direct vision
- PMID: 40804674
- PMCID: PMC12351962
- DOI: 10.1186/s12893-025-02982-x
Clinical efficacy analysis of LNG-IUS tail anchoring to the superficial myometrium under hysteroscopic direct vision
Abstract
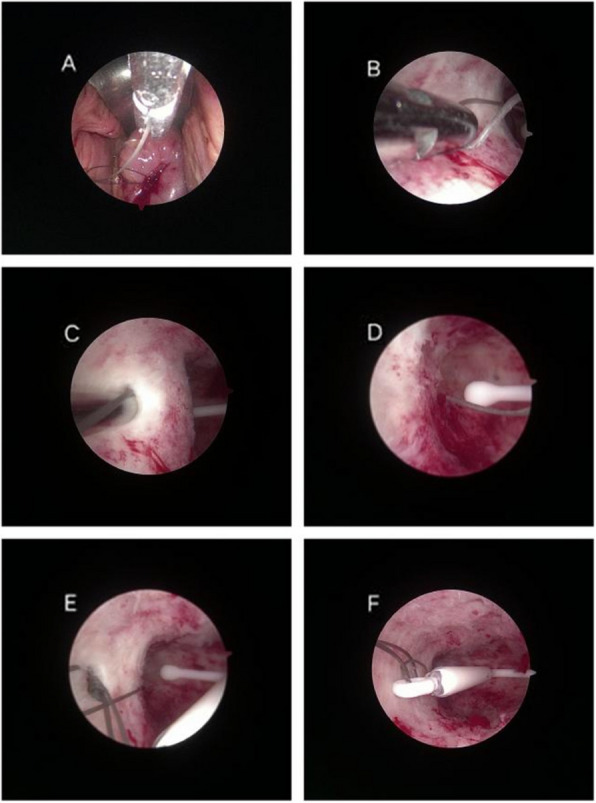
Objective: To investigate the clinical efficacy of levonorgestrel-releasing intrauterine system (LNG-IUS) tail anchoring to the superficial myometrium under hysteroscopic direct vision.
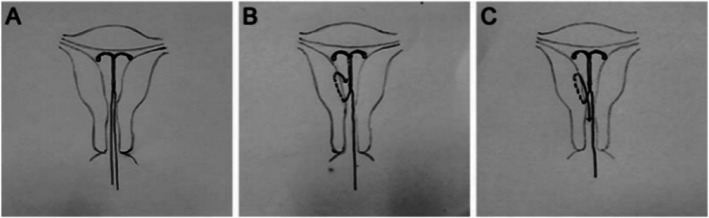
Methods: From March 1, 2017, to March 1, 2022, 206 patients at the Third Xiangya Hospital of Central South University who had a history of at least one LNG-IUS expulsion and who required replacement of the LNG-IUS were retrospectively analyzed. Patients were divided into a common placement group and an anchoring group according to the placement method used for the LNG-IUS. Between-group comparisons of the re-expulsion rate and adverse reactions were performed, and the clinical efficacy of anchoring was evaluated. The patients in the anchoring group were divided into short-tail and long-tail groups on the basis of the length of the tail.
Results: After propensity score matching (PSM), the re-expulsion rate was 18.87% for the anchoring group and 43.40% for the common placement group. There was a significant difference in re-expulsion rates between the two groups (P< 0.05), with the anchoring group having a significantly lower rate than the common placement group. Additionally, the re-expulsion rate of the long-tail group (6.90%) was significantly lower than that of the short-tail group (28.77%) (P< 0.05). The use of anchoring surgery did not lead to a higher incidence of uterine perforation or infection.
Conclusions: For patients with a history of levonorgestrel-releasing intrauterine system expulsion, anchoring the LNG-IUS tail in the superficial uterine myometrium under hysteroscopy can effectively prevent re-expulsion and significantly reduce the re-expulsion rate, especially when the long tail anchoring method is used. This technique is efficacious and warrants widespread adoption.
Keywords: Anchoring surgery; Clinical efficacy; Expulsion; LNG-IUS.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was approved by the Third Xiangya Hospital of Central South University Institutional Review Board, approval number 24301. Consent for publication: Informed consent was obtained from all individual participants included in the study. The participants were provided with detailed information regarding the study’s purpose, procedures, risks, and benefits, and they were given the opportunity to ask questions before providing their consent. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding.Cochrane Database Syst Rev. 2005 Oct 19;(4):CD002126. doi: 10.1002/14651858.CD002126.pub2. Cochrane Database Syst Rev. 2005. Update in: Cochrane Database Syst Rev. 2015 Apr 30;(4):CD002126. doi: 10.1002/14651858.CD002126.pub3. PMID: 16235297 Updated.
-
Surgery versus medical therapy for heavy menstrual bleeding.Cochrane Database Syst Rev. 2016 Jan 29;2016(1):CD003855. doi: 10.1002/14651858.CD003855.pub3. Cochrane Database Syst Rev. 2016. PMID: 26820670 Free PMC article.
-
Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding.Cochrane Database Syst Rev. 2015 Apr 30;(4):CD002126. doi: 10.1002/14651858.CD002126.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2020 Jun 12;6:CD002126. doi: 10.1002/14651858.CD002126.pub4. PMID: 25924648 Updated.
-
Hormonally impregnated intrauterine systems (IUSs) versus other forms of reversible contraceptives as effective methods of preventing pregnancy.Cochrane Database Syst Rev. 2004;2004(3):CD001776. doi: 10.1002/14651858.CD001776.pub2. Cochrane Database Syst Rev. 2004. PMID: 15266453 Free PMC article.
-
Immediate postpartum insertion of intrauterine device for contraception.Cochrane Database Syst Rev. 2015 Jun 26;2015(6):CD003036. doi: 10.1002/14651858.CD003036.pub3. Cochrane Database Syst Rev. 2015. PMID: 26115018 Free PMC article.
References
-
- Lang JH, Leng JH, Deng S, et al. Chinese expert panel consensus recommendations on the clinical application of China levonorgestrel-releasing intrauterine system. Chinese Journal of Obstetrics and Gynecology. 2019;54(12):815–25. 10.3760/cma.j.issn.0529-567x.2019.12.005. - PubMed
-
- Li L, Leng JH, Jia SZ, et al. Analysis of unplanned taking-out and expulsion of LNG-IUS and related factors during the treatment of symptomatic adenomyosis. Chinese Journal of Practical Gynecology and Obstetrics. 2016;32(11):1088–92.
-
- Jin YN, Li HJ, Kim SK, et al. Factors affecting the spontaneous expulsion of the levonorgestrel-releasing intrauterine system. Int J Gynecol Obstet. 2014;126(2):165–9. 10.1016/j.ijgo.2014.02.017. - PubMed
-
- Park DS, Kim ML, Song TJ, et al. Clinical experiences of the levonorgestrel-releasing intrauterine system in patients with large symptomatic adenomyosis. Taiwan J Obstet Gynecol. 2015;54(4):412–5. 10.1016/j.tjog.2014.05.009. - PubMed
-
- Lee JS, Hong GY, Park BJ, et al. Ultrasound-guided high-intensity focused ultrasound treatment for uterine fibroid & adenomyosis: A single center experience from the Republic of Korea. Ultrason Sonochem. 2015;27:682–7. 10.1016/j.ultsonch.2015.05.033. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
