

Multimodality Imaging in Aldosterone-Induced Cardiomyopathy: Early Detection and Prognostic Implications
- PMID: 40804860
- PMCID: PMC12345877
- DOI: 10.3390/diagnostics15151896
Multimodality Imaging in Aldosterone-Induced Cardiomyopathy: Early Detection and Prognostic Implications
Abstract
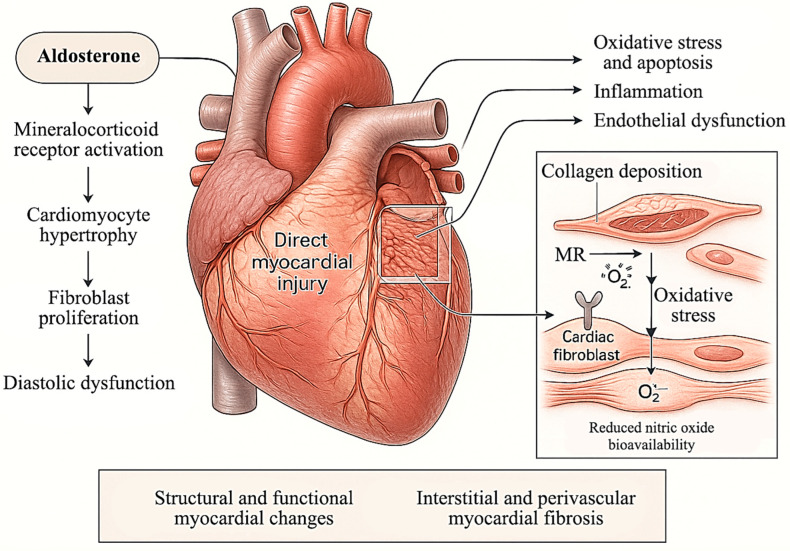
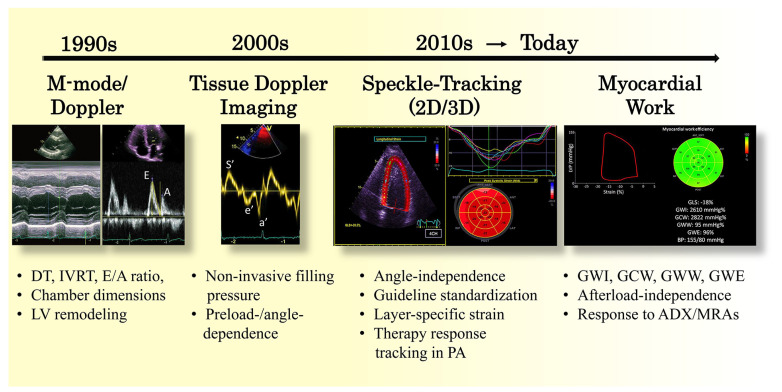
Primary aldosteronism (PA), the most common cause of secondary hypertension, is increasingly recognized as an independent driver of adverse cardiac remodeling, mediated through mechanisms beyond elevated blood pressure alone. Chronic aldosterone excess leads to myocardial fibrosis, left ventricular hypertrophy, and diastolic dysfunction via mineralocorticoid receptor activation, oxidative stress, inflammation, and extracellular matrix dysregulation. These changes culminate in a distinct cardiomyopathy phenotype, often underrecognized in early stages. Multimodality cardiac imaging, led primarily by conventional and speckle-tracking echocardiography, and complemented by exploratory cardiac magnetic resonance (CMR) techniques such as T1 mapping and late gadolinium enhancement, enables non-invasive assessment of structural, functional, and tissue-level changes in aldosterone-mediated myocardial damage. While numerous studies have established the diagnostic and prognostic relevance of imaging in PA, several gaps remain. Specifically, the relative sensitivity of different modalities in detecting subclinical myocardial changes, the long-term prognostic significance of imaging biomarkers, and the differential impact of adrenalectomy versus medical therapy on cardiac reverse remodeling require further clarification. Moreover, the lack of standardized imaging-based criteria for defining and monitoring PA-related cardiomyopathy hinders widespread clinical implementation. This narrative review aims to synthesize current knowledge on the pathophysiological mechanisms of aldosterone-induced cardiac remodeling, delineate the strengths and limitations of existing imaging modalities, and critically evaluate the comparative effects of surgical and pharmacologic interventions. Emphasis is placed on early detection strategies, identification of imaging biomarkers with prognostic utility, and integration of multimodal imaging into clinical decision-making pathways. By outlining current evidence and highlighting key unmet needs, this review provides a framework for future research aimed at advancing personalized care and improving cardiovascular outcomes in patients with PA.
Keywords: adrenalectomy; cardiac magnetic resonance; cardiac remodeling; echocardiography; left ventricular hypertrophy; mineralocorticoid receptor antagonists; primary aldosteronism.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Systematic review and modelling of the cost-effectiveness of cardiac magnetic resonance imaging compared with current existing testing pathways in ischaemic cardiomyopathy.Health Technol Assess. 2014 Sep;18(59):1-120. doi: 10.3310/hta18590. Health Technol Assess. 2014. PMID: 25265259 Free PMC article.
-
Primary Aldosteronism: An Endocrine Society Clinical Practice Guideline.J Clin Endocrinol Metab. 2025 Aug 7;110(9):2453-2495. doi: 10.1210/clinem/dgaf284. J Clin Endocrinol Metab. 2025. PMID: 40658480
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
-
Systemic Inflammatory Response Syndrome.2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jun 20. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31613449 Free Books & Documents.
References
-
- Rossi G.P., Bernini G., Caliumi C., Desideri G., Fabris B., Ferri C., Ganzaroli C., Giacchetti G., Letizia C., Maccario M., et al. A prospective study of the prevalence of primary aldosteronism in 1125 hypertensive patients. J. Am. Coll. Cardiol. 2006;48:2293–2300. doi: 10.1016/j.jacc.2006.07.059. - DOI - PubMed
-
- Monticone S., Burrello J., Tizzani D., Bertello C., Viola A., Buffolo F., Gabetti L., Mengozzi G., Williams T.A., Rabbia F., et al. Prevalence and Clinical Manifestations of Primary Aldosteronism Encountered in Primary Care Practice. J. Am. Coll. Cardiol. 2017;69:1811–1820. doi: 10.1016/j.jacc.2017.01.052. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
