

Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria
- PMID: 40804872
- PMCID: PMC12346232
- DOI: 10.3390/diagnostics15151908
Prevalence of Temporomandibular Disorder Symptoms Among Dental Students at the Faculty of Dental Medicine in Iași: A Self-Reported Study Based on DC/TMD Criteria
Abstract
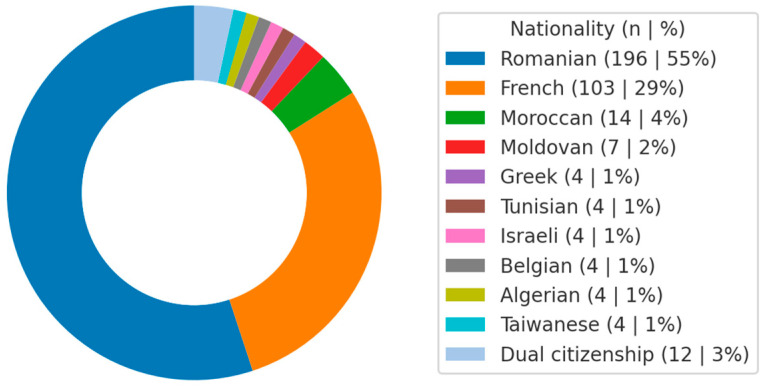
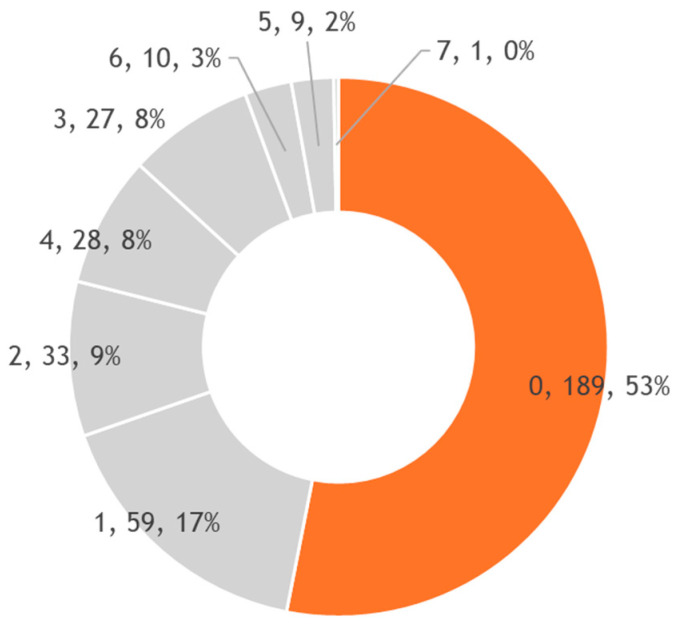
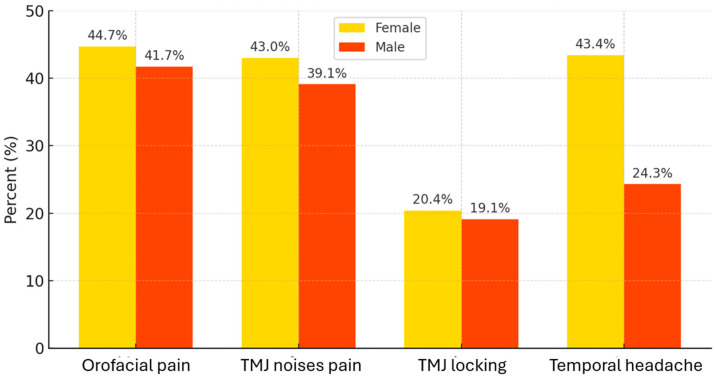
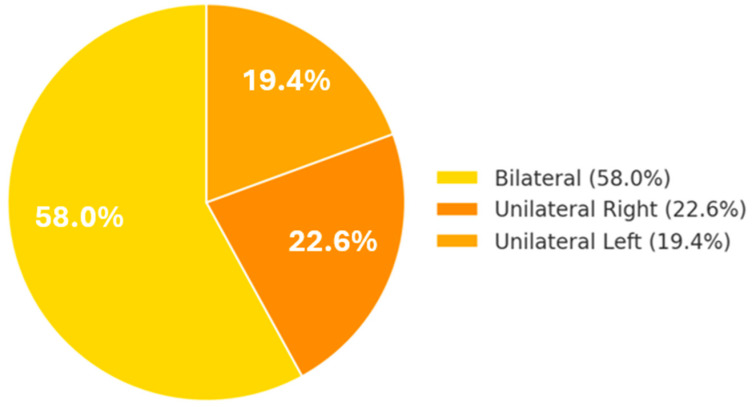
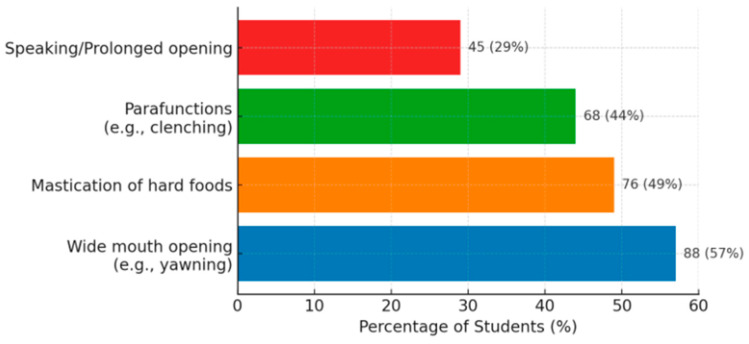
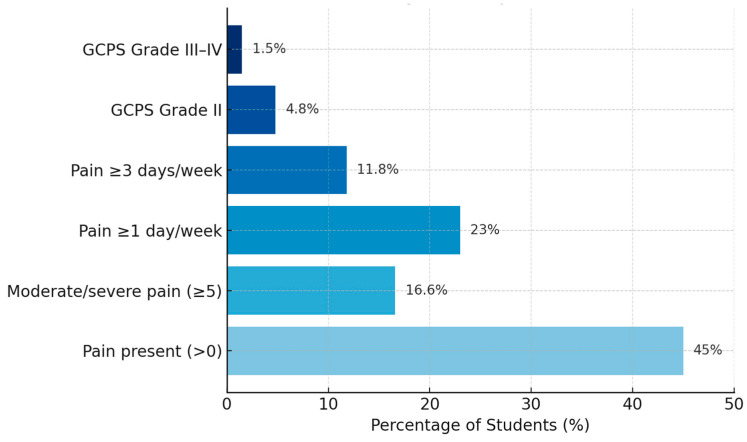
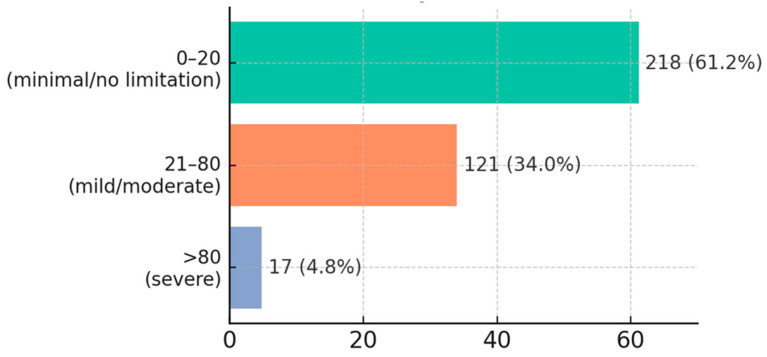
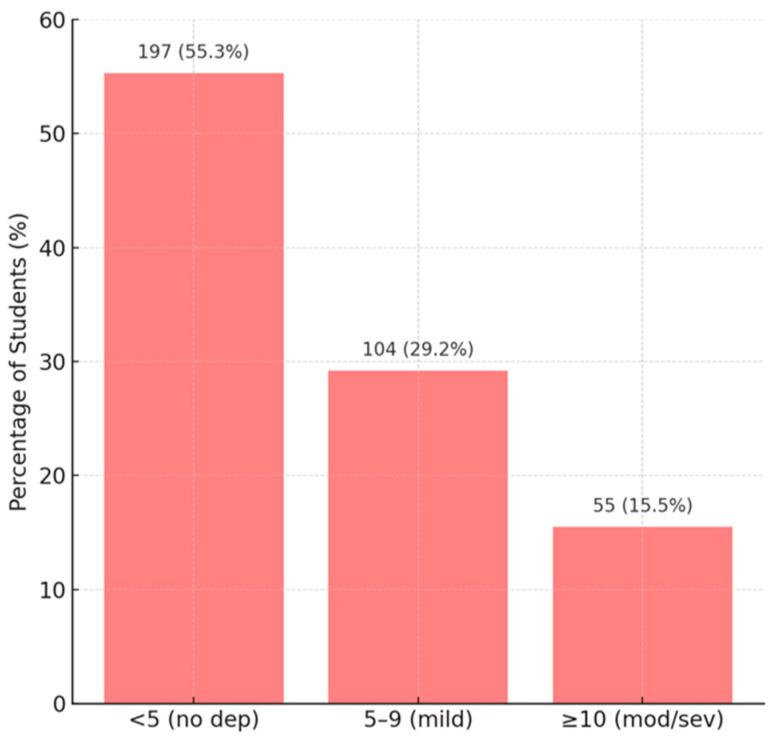
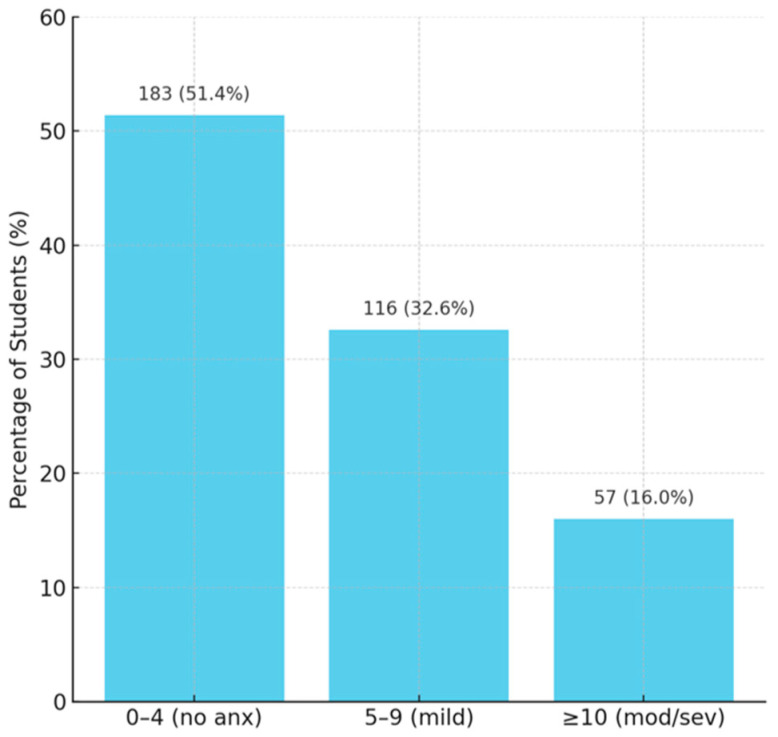
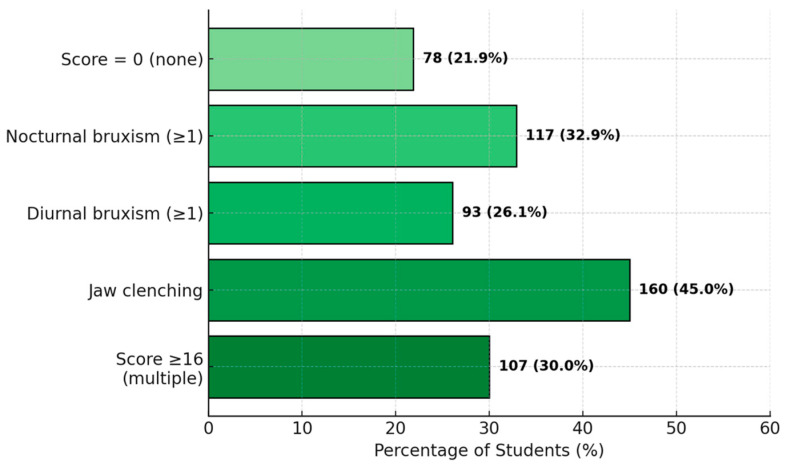
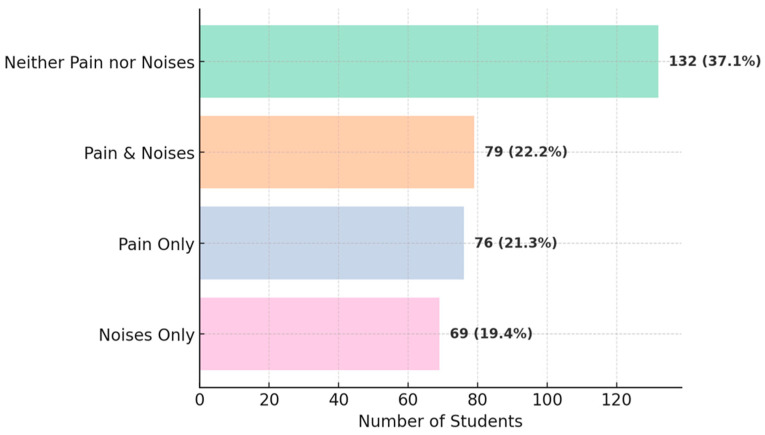
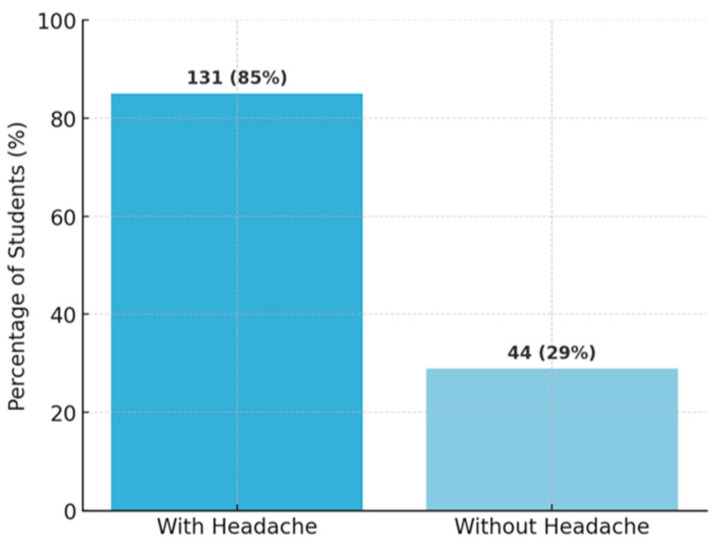
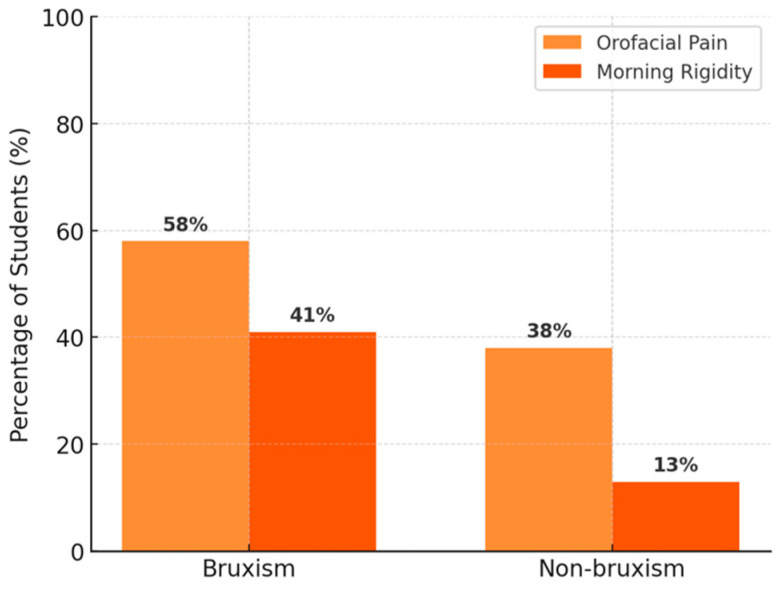
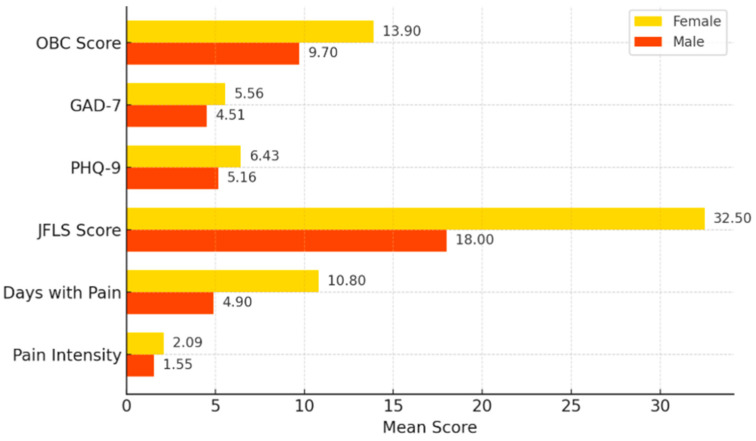
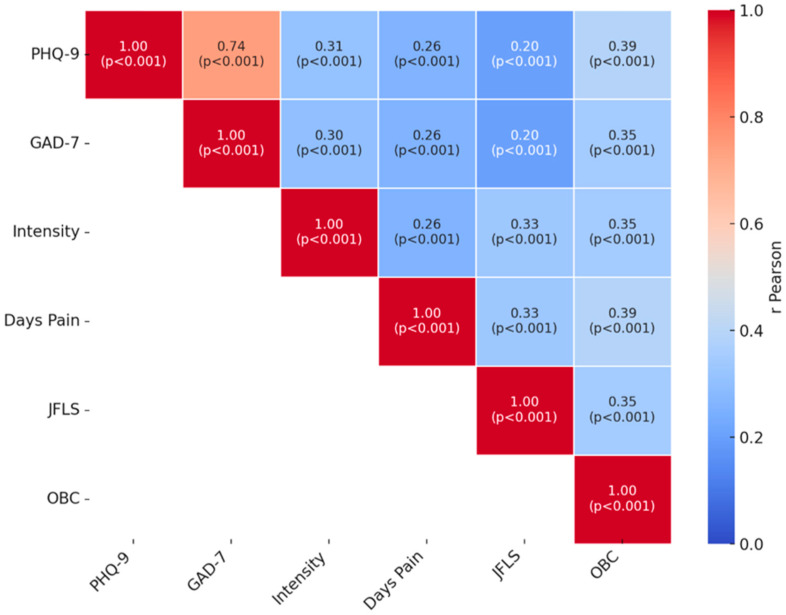
Temporomandibular disorders (TMDs) encompass a heterogeneous group of musculoskeletal and neuromuscular conditions affecting the temporomandibular joint (TMJ) and masticatory system. Due to academic stress and parafunctional habits, dental students may be particularly vulnerable to TMD. Objective: To determine the prevalence of TMD symptoms and their psychosocial and functional correlates among students at the Faculty of Dental Medicine, UMPh Iasi, Romania, using the diagnostic criteria for TMD (DC/TMD) self-report axis and axis II instruments. Methods: In this cross-sectional survey, 356 volunteer students (66.0% female; mean age, 22.9 ± 3.6 years) out of a total population of 1874 completed an online DC/TMD-based questionnaire. Axis I assessed orofacial pain, joint noises, and mandibular locking. Axis II instruments included the Graded Chronic Pain Scale (GCPS), Jaw Functional Limitation Scale (JFLS-20), Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), and Oral Behaviors Checklist (OBC). Descriptive statistics summarized frequencies, means, and standard deviations; χ2 tests and t-tests compared subgroups by sex; Pearson correlations explored relationships among continuous measures (α = 0.05). Results: A total of 5% of respondents reported orofacial pain in the past 30 days; 41.6% observed TMJ noises; 19.7% experienced locking episodes. Mean JFLS score was 28.3 ± 30.5, with 4.8% scoring > 80 (severe limitation). Mean PHQ-9 was 5.96 ± 5.37 (mild depression); 15.5% scored ≥ 10. Mean GAD-7 was 5.20 ± 4.95 (mild anxiety); 16.0% scored ≥ 10. Mean OBC score was 12.3 ± 8.5; 30.1% scored ≥ 16, indicating frequent parafunctional habits. Symptom prevalence was similar by sex, except temporal headache (43.4% females vs. 24.3% males; p = 0.0008). Females reported higher mean scores for pain intensity (2.09 vs. 1.55; p = 0.0013), JFLS (32.5 vs. 18.0; p < 0.001), PHQ-9 (6.43 vs. 5.16; p = 0.048), and OBC (13.9 vs. 9.7; p = 0.0014). Strong correlation was observed between PHQ-9 and GAD-7 (r = 0.74; p < 0.001); moderate correlations were observed between pain intensity and PHQ-9 (r = 0.31) or GAD-7 (r = 0.30), between JFLS and pain intensity (r = 0.33), and between OBC and PHQ-9 (r = 0.39) (all p < 0.001). Conclusions: Nearly half of dental students reported TMD symptoms, with appreciable functional limitation and psychosocial impact. Parafunctional behaviors and psychological distress were significantly associated with pain and dysfunction. These findings underscore the need for early screening, stress-management interventions, and interdisciplinary care strategies in the dental student population.
Keywords: DC/TMD; dental students; psychosocial factors; temporomandibular disorders prevalence.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Prevalence of Signs and Symptoms of Temporomandibular Disorders and Their Association with Emotional Factors and Waking-State Oral Behaviors on University Students: A Cross-Sectional Study.Healthcare (Basel). 2025 Jun 12;13(12):1414. doi: 10.3390/healthcare13121414. Healthcare (Basel). 2025. PMID: 40565441 Free PMC article.
-
The Impact of Parafunctional Habits on Temporomandibular Disorders in Medical Students.J Clin Med. 2025 Jul 27;14(15):5301. doi: 10.3390/jcm14155301. J Clin Med. 2025. PMID: 40806923 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Psychological therapies for temporomandibular disorders (TMDs).Cochrane Database Syst Rev. 2022 Aug 11;8(8):CD013515. doi: 10.1002/14651858.CD013515.pub2. Cochrane Database Syst Rev. 2022. PMID: 35951347 Free PMC article.
-
Occlusal interventions for managing temporomandibular disorders.Cochrane Database Syst Rev. 2024 Sep 16;9(9):CD012850. doi: 10.1002/14651858.CD012850.pub2. Cochrane Database Syst Rev. 2024. PMID: 39282765
References
-
- Ohrbach R., Sharma S. Temporomandibular disorders: Definition and etiology. Semin. Orthod. 2024;30:237–242. doi: 10.1053/j.sodo.2023.12.011. - DOI
-
- De Leeuw R., Klasser G.D. Orofacial pain: Guidelines for assessment, diagnosis, and management. Am. J. Orthod. Dentofac. Orthop. 2008;134:171. doi: 10.25241/stomaeduj.2015.2(2).bookreview.6. - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous
