

Variations in the Diagnosis and Management of Benign Paroxysmal Positional Vertigo Among Physician Specialties in Saudi Arabia: Influence of Clinical Experience and Case Exposure
- PMID: 40805918
- PMCID: PMC12345922
- DOI: 10.3390/healthcare13151887
Variations in the Diagnosis and Management of Benign Paroxysmal Positional Vertigo Among Physician Specialties in Saudi Arabia: Influence of Clinical Experience and Case Exposure
Abstract
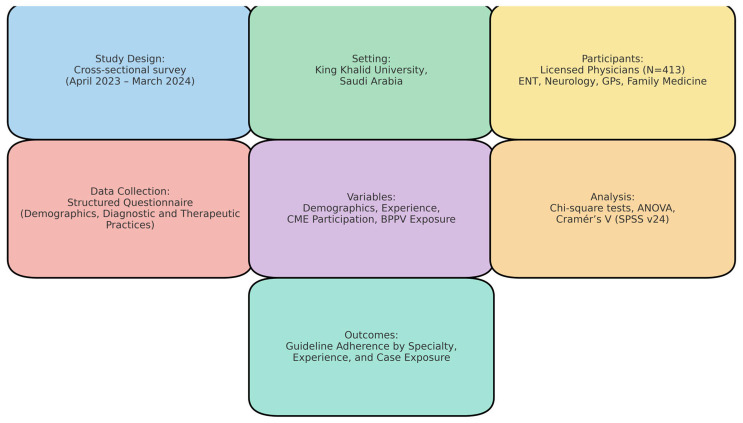
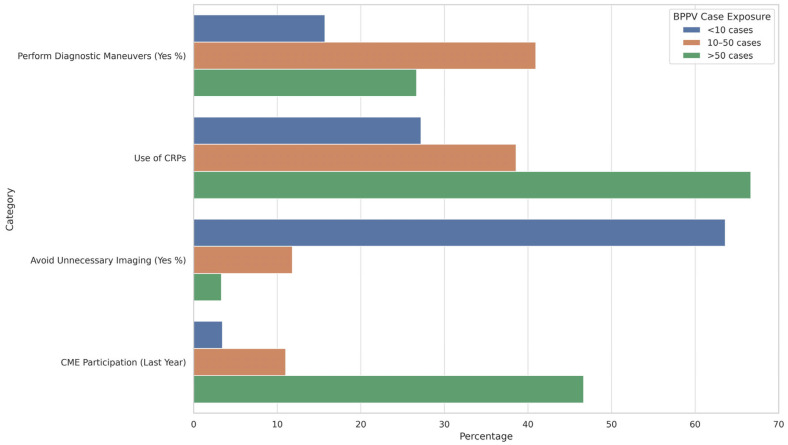
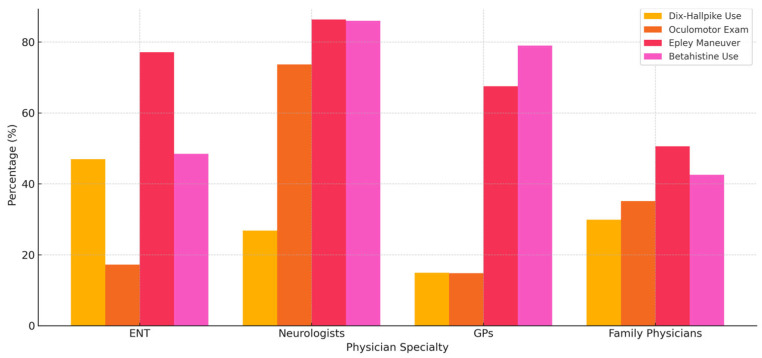
Background/Objectives: Benign paroxysmal positional vertigo (BPPV) is the most prevalent vestibular disorder encountered in clinical settings and is highly responsive to evidence-based diagnostic and therapeutic interventions. However, variations in practice patterns among physician specialties can compromise timely diagnosis and effective treatment. Understanding these variations is essential for improving clinical outcomes and standardizing care. This study aimed to assess the diagnostic and treatment practices for BPPV among Ear, Nose, and Throat (ENT) specialists, neurologists, general practitioners, and family physicians in Saudi Arabia and to examine how these practices are influenced by clinical experience and patient case exposure. Methods: A cross-sectional, questionnaire-based study was conducted between April 2023 and March 2024 at King Khalid University, Abha, Saudi Arabia. A total of 413 physicians were recruited using purposive sampling. Data were analyzed using IBM SPSS version 24.0. Parametric tests, including one-way ANOVA and chi-square tests, were used to assess differences across groups. A p-value of <0.05 was considered statistically significant. Results: Overall, all physician groups exhibited limited adherence to guideline-recommended positional diagnostic and therapeutic maneuvers. However, ENT specialists and neurologists demonstrated relatively higher compliance, particularly in performing the Dix-Hallpike test, with 46.97% and 26.79% reporting "always" using the maneuver, respectively (p < 0.001, Cramér's V = 0.22). Neurologists were the most consistent in conducting oculomotor examinations, with 73.68% reporting routine performance (p < 0.001, Cramér's V = 0.35). Epley maneuver usage was highest among neurologists (86.36%) and ENT specialists (77.14%) compared to family physicians (50.60%) and GPs (67.50%) (p = 0.044). Physicians with 11-15 years of experience and >50 BPPV case exposures consistently showed a greater use of diagnostic maneuvers, repositioning techniques, and guideline-concordant medication use (betahistine 76.67%; p < 0.001). Continuing medical education (CME) participation and the avoidance of unnecessary imaging were also highest in this group (46.67% and 3.33%, respectively; p < 0.001). Conclusions: Significant inter-specialty differences exist in the management of BPPV in Saudi Arabia. Greater clinical experience and higher case exposure are associated with improved adherence to evidence-based practices. Targeted educational interventions are needed, particularly in primary care, to enhance guideline implementation.
Keywords: Benign paroxysmal positional vertigo; canalith repositioning; clinical experience; diagnostic maneuvers; physician specialties.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Modifications of the Epley (canalith repositioning) manoeuvre for posterior canal benign paroxysmal positional vertigo (BPPV).Cochrane Database Syst Rev. 2012 Apr 18;2012(4):CD008675. doi: 10.1002/14651858.CD008675.pub2. Cochrane Database Syst Rev. 2012. PMID: 22513962 Free PMC article.
-
The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo.Cochrane Database Syst Rev. 2014 Dec 8;2014(12):CD003162. doi: 10.1002/14651858.CD003162.pub3. Cochrane Database Syst Rev. 2014. PMID: 25485940 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Minimal Stimulus Strategy in Benign Paroxysmal Positional Vertigo: Its Application in a Resource Limited Setting.Indian J Otolaryngol Head Neck Surg. 2024 Dec;76(6):5740-5745. doi: 10.1007/s12070-024-05081-0. Epub 2024 Sep 24. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 39559098
-
Betahistine for symptoms of vertigo.Cochrane Database Syst Rev. 2016 Jun 21;2016(6):CD010696. doi: 10.1002/14651858.CD010696.pub2. Cochrane Database Syst Rev. 2016. PMID: 27327415 Free PMC article.
References
-
- Savaş Ö., Cüreoğlu S., Güneri E.A. Neurotology Updates. Springer; Berlin/Heidelberg, Germany: 2024. Benign paroxysmal positional vertigo; pp. 91–136.
-
- Micarelli A., Viziano A., Granito I., Arena M., Maurizi R., Micarelli R.X., Alessandrini M. Onset and resolution failure of recurrent benign paroxysmal positional vertigo: The role of cervical range of motion. Eur. Arch. Oto-Rhino-Laryngol. 2022;279:2183–2192. doi: 10.1007/s00405-021-07226-1. - DOI - PubMed
-
- Vanni S., Vannucchi P., Pecci R., Pepe G., Paciaroni M., Pavellini A., Ronchetti M., Pelagatti L., Bartolucci M., Konze A. Consensus paper on the management of acute isolated vertigo in the emergency department. Intern. Emerg. Med. 2024;19:1181–1202. doi: 10.1007/s11739-024-03664-x. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
