

Electromagnetic Transduction Therapy (EMTT) Enhances Tenocyte Regenerative Potential: Evidence for Senolytic-like Effects and Matrix Remodeling
- PMID: 40806255
- PMCID: PMC12346084
- DOI: 10.3390/ijms26157122
Electromagnetic Transduction Therapy (EMTT) Enhances Tenocyte Regenerative Potential: Evidence for Senolytic-like Effects and Matrix Remodeling
Abstract
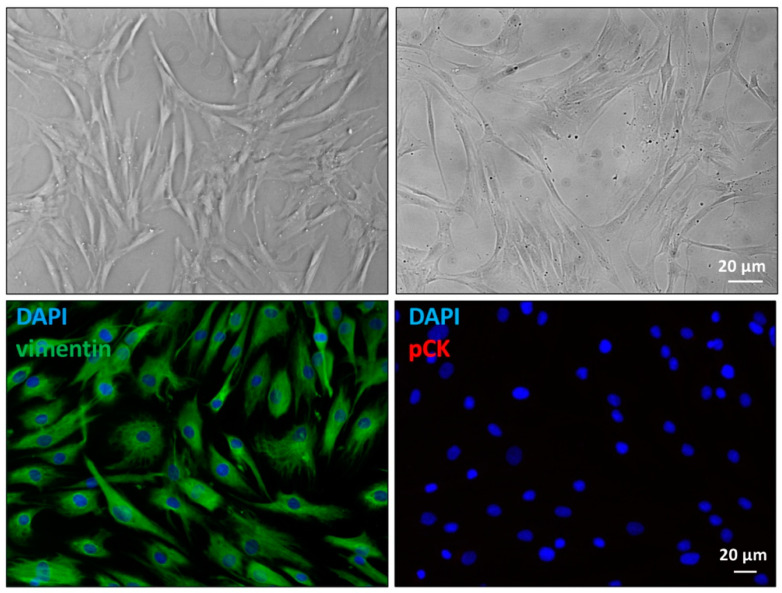
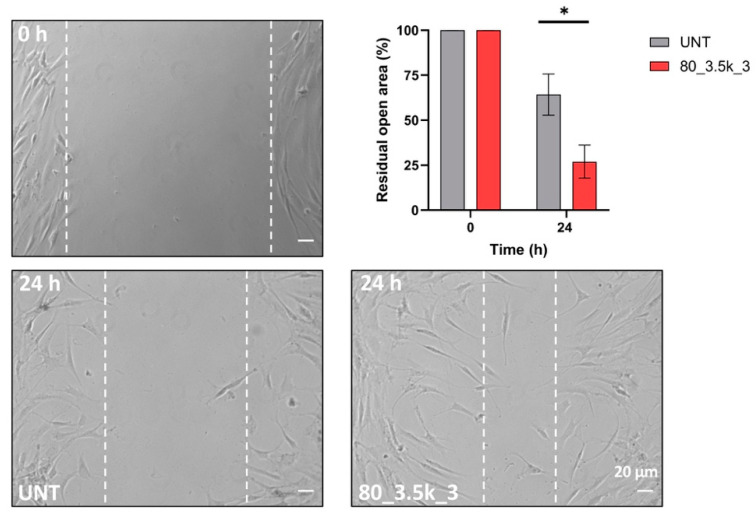
Tendinopathies are a significant challenge in musculoskeletal medicine, with current treatments showing variable efficacy. Electromagnetic transduction therapy (EMTT) has emerged as a promising therapeutic approach, but its biological effects on tendon cells remain largely unexplored. Here, we investigated the effects of EMTT on primary cultured human tenocytes' behavior and functions in vitro, focusing on cellular responses, senescence-related pathways, and molecular mechanisms. Primary cultures of human tenocytes were established from semitendinosus tendon biopsies of patients undergoing anterior cruciate ligament (ACL) reconstruction (n = 6, males aged 17-37 years). Cells were exposed to EMTT at different intensities (40 and 80 mT) and impulse numbers (1000-10,500). Cell viability (MTT assay), proliferation (Ki67), senescence markers (CDKN2a/INK4a), migration (scratch test), cytoskeleton organization (immunofluorescence), and gene expression (RT-PCR) were analyzed. A 40 mT exposure elicited minimal effects, whereas 80 mT treatments induced significant cellular responses. Repeated 80 mT exposure demonstrated a dual effect: despite a moderate decrease in overall cell vitality, increased Ki67 expression (+7%, p ≤ 0.05) and significant downregulation of senescence marker CDKN2a/INK4a were observed, suggesting potential senolytic-like activity. EMTT significantly enhanced cell migration (p < 0.001) and triggered cytoskeletal remodeling, with amplified stress fiber formation and paxillin redistribution. Molecular analysis revealed upregulation of tenogenic markers (Scleraxis, Tenomodulin) and enhanced Collagen I and III expressions, particularly with treatments at 80 mT, indicating improved matrix remodeling capacity. EMTT significantly promotes tenocyte proliferation, migration, and matrix production, while simultaneously exhibiting senolytic-like effects through downregulation of senescence-associated markers. These results support EMTT as a promising therapeutic approach for the management of tendinopathies through multiple regenerative mechanisms, though further studies are needed to validate these effects in vivo.
Keywords: EMTT; cell migration; extracellular matrix remodeling; human tenocytes; mechanotransduction; senescence; senolytic; tendinopathy; tendon regeneration.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
