

Prevalence and Levels of Thyroid Autoantibodies in Polycystic Ovary Syndrome-Impact of TSH- and BMI-Matched Comparisons: A Systematic Review and Meta-Analysis
- PMID: 40806651
- PMCID: PMC12347112
- DOI: 10.3390/ijms26157525
Prevalence and Levels of Thyroid Autoantibodies in Polycystic Ovary Syndrome-Impact of TSH- and BMI-Matched Comparisons: A Systematic Review and Meta-Analysis
Abstract
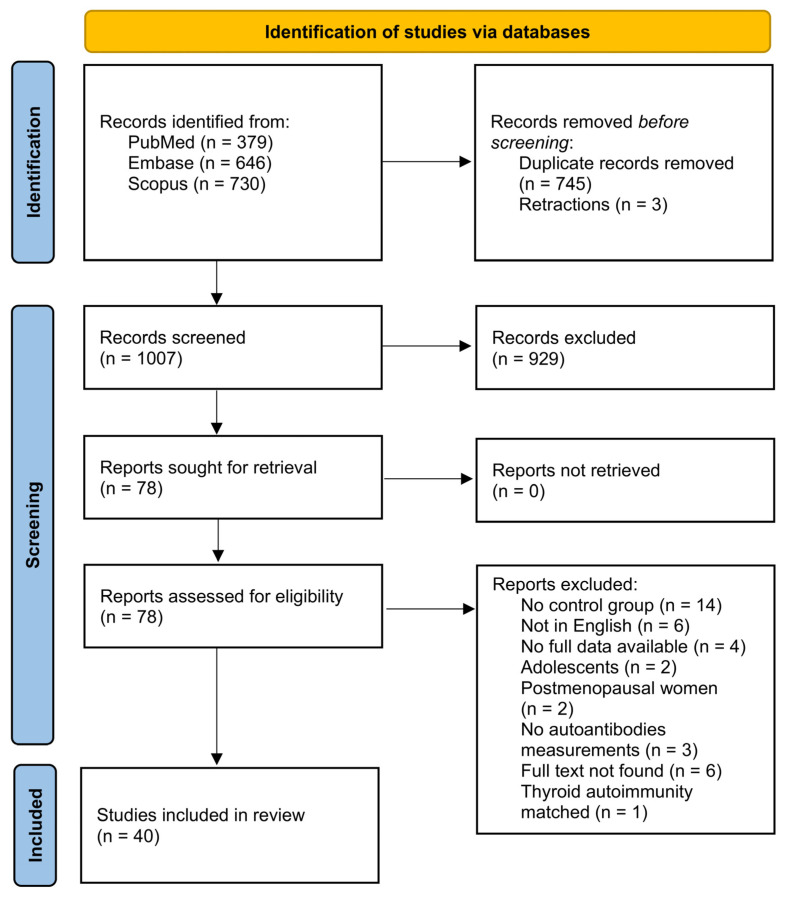
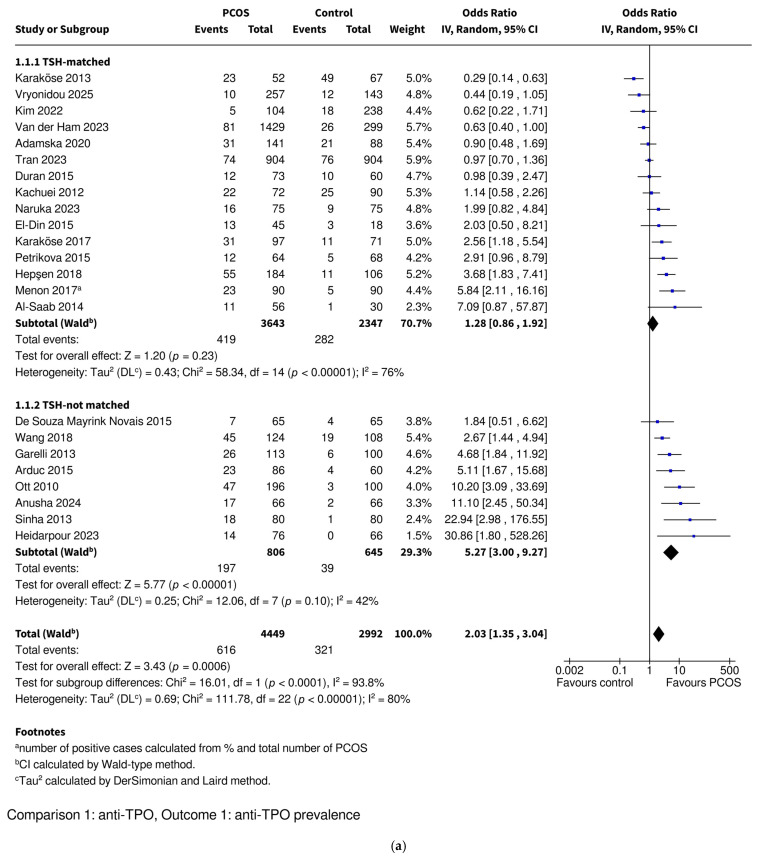
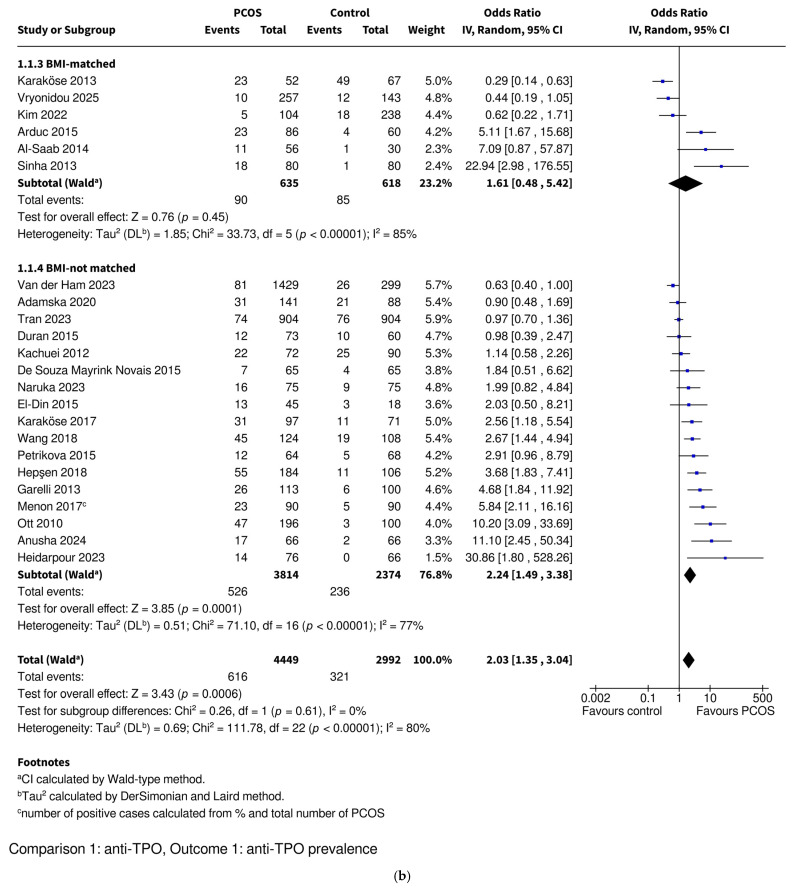
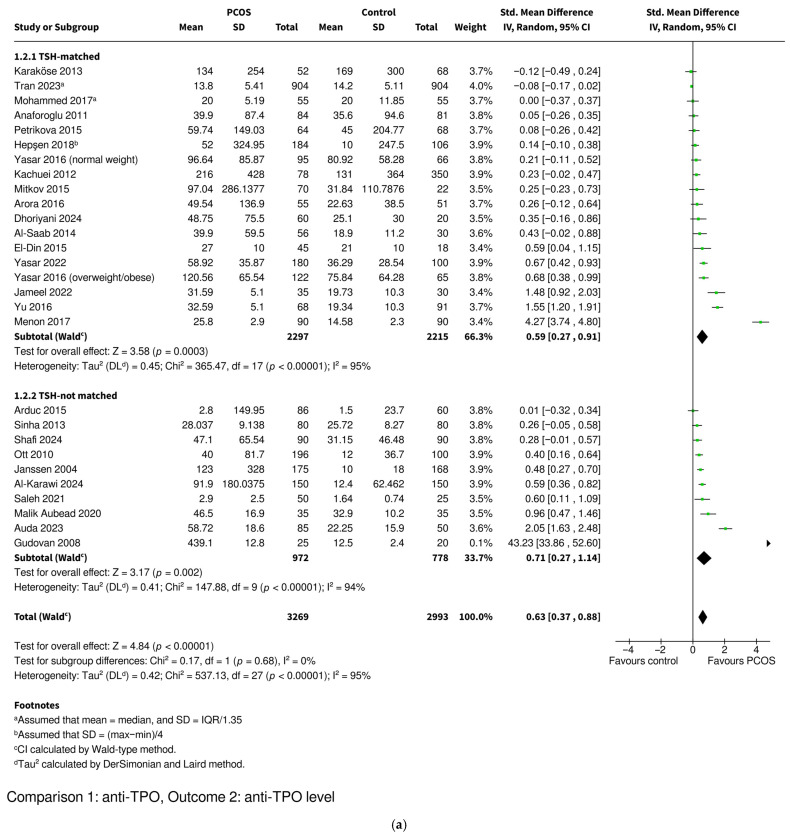
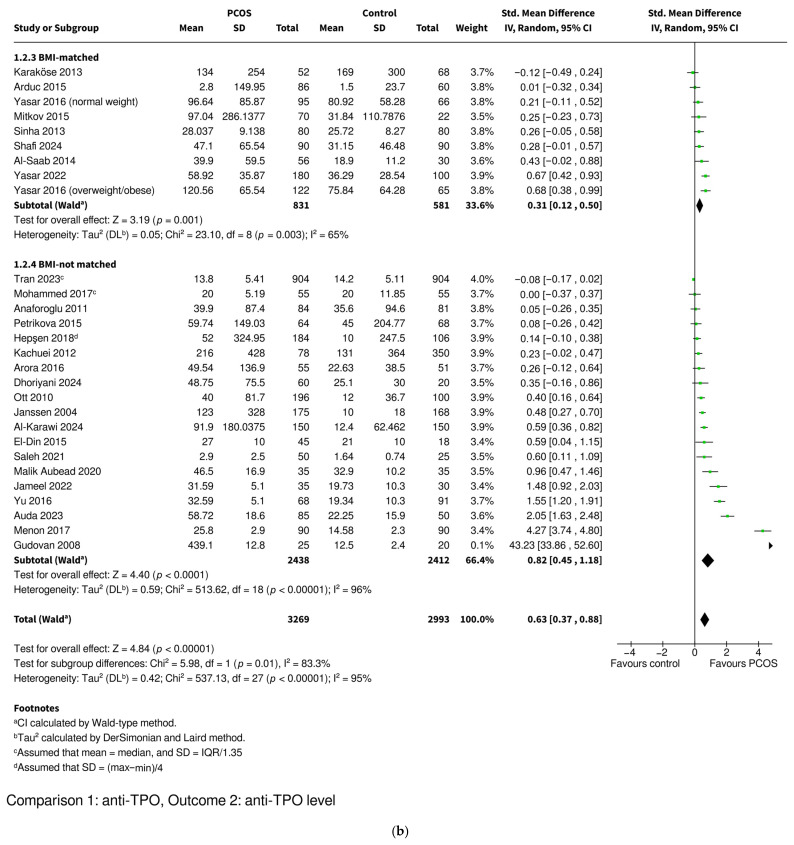
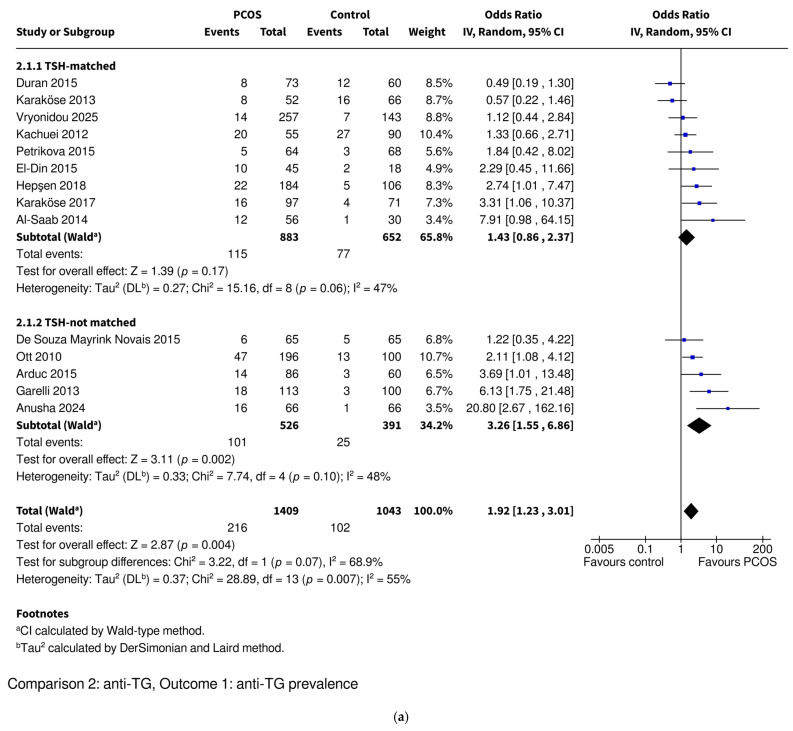
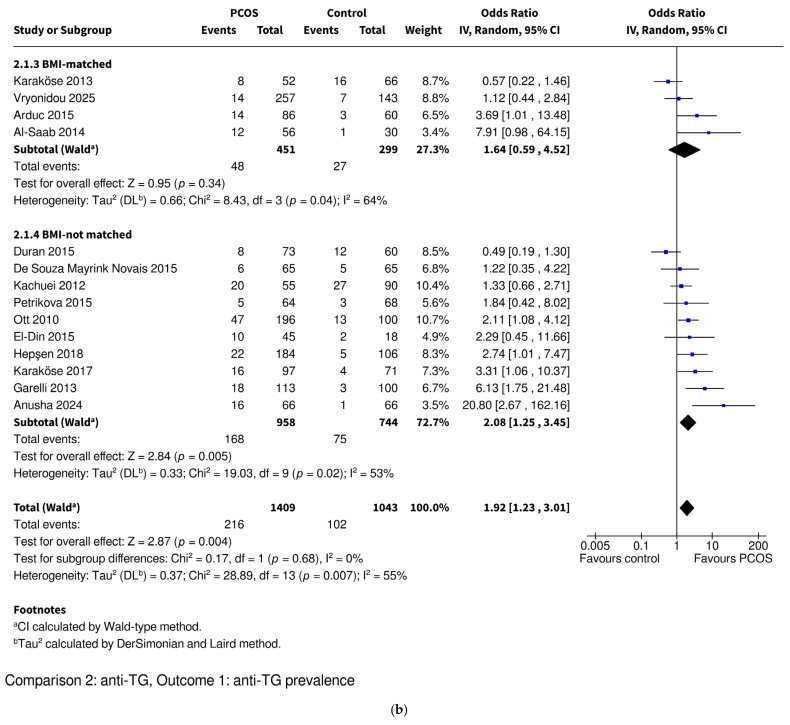
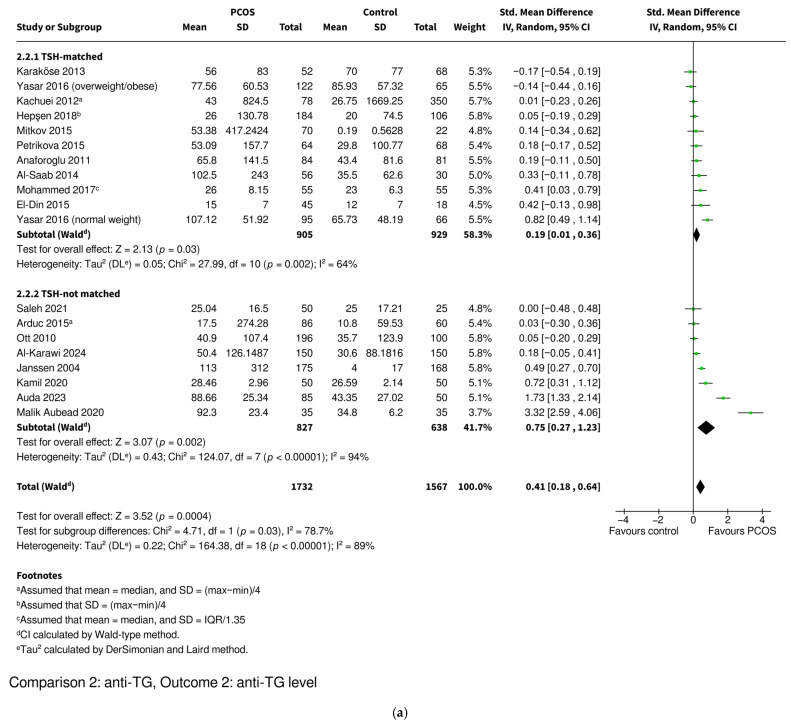
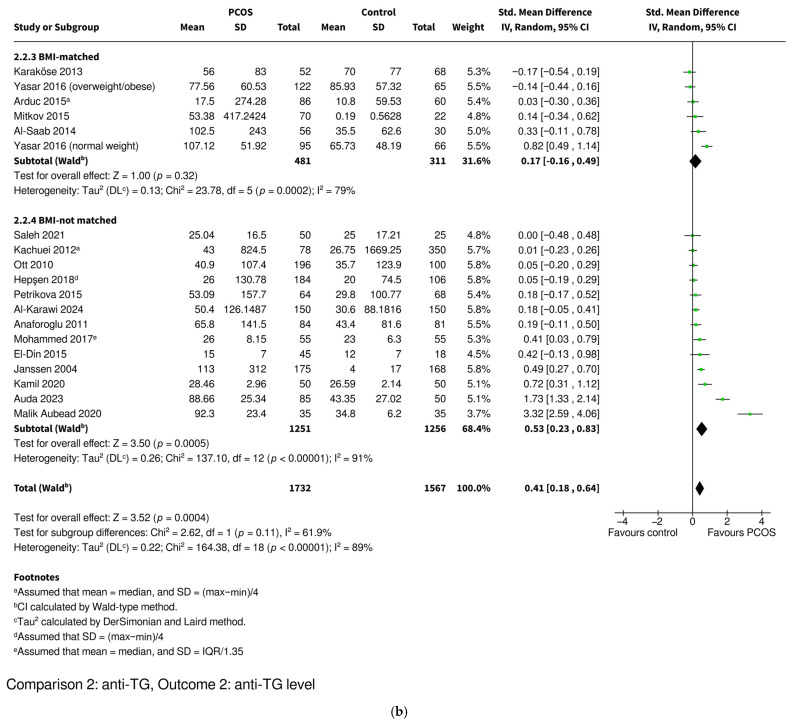
Polycystic ovary syndrome (PCOS) is a complex condition affecting women of reproductive age, characterized by menstrual irregularities, hyperandrogenism, polycystic ovarian morphology, and low-grade inflammation accompanied by oxidative stress and increased autoimmune risk, particularly Hashimoto's thyroiditis. Many studies have examined thyroid autoantibodies-anti-thyroid peroxidase antibodies (anti-TPO) and anti-thyroglobulin antibodies (anti-TG)-in PCOS; however, observed differences in baseline thyroid-stimulating hormone (TSH) levels and body mass indices (BMIs) impede a direct interpretation of the results. This systematic review and meta-analysis aimed to summarize the available evidence on the prevalence and levels of anti-TPO and anti-TG in women with PCOS. We conducted a systematic search of PubMed, Scopus, and Embase, which yielded 40 eligible, observational studies including 6045 women with PCOS and 4527 controls. Subgroup analyses were conducted separately for TSH- and BMI-matched populations. Anti-TPO prevalence (odds ratio [OR] = 2.03; 95% confidence interval [CI]: 1.35-3.04; p = 0.0006) and levels (standardized mean difference [SMD] = 0.63; 95% CI: 0.37-0.88; p < 0.00001) were significantly higher in PCOS patients. Anti-TG prevalence (OR = 1.92; 95% CI: 1.23-3.01; p = 0.004) and levels (SMD = 0.41; 95% CI: 0.18-0.64; p = 0.0004) were also significantly elevated. In matched subgroups, prevalence differences were no longer significant, though anti-TPO levels remained significantly elevated and anti-TG levels were borderline significant in the TSH-matched subgroup of PCOS women. Although differences in thyroid autoantibody prevalence in women with PCOS appear to be driven by elevated TSH levels and BMIs, the persistently increased antibody levels in the majority of matched subgroups suggest that PCOS itself may contribute independently to heightened autoimmune activation.
Keywords: Hashimoto’s thyroiditis; PCOS; anti-TG; anti-TPO; anti-thyroglobulin antibodies; anti-thyroid peroxidase antibodies; antibodies; autoimmune thyroid disease; autoimmunity; polycystic ovary syndrome.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
High prevalence of moderate and severe depressive and anxiety symptoms in polycystic ovary syndrome: a systematic review and meta-analysis.Hum Reprod. 2017 May 1;32(5):1075-1091. doi: 10.1093/humrep/dex044. Hum Reprod. 2017. PMID: 28333286
-
Ovarian surgery for symptom relief in women with polycystic ovary syndrome.Cochrane Database Syst Rev. 2017 Nov 10;11(11):CD009526. doi: 10.1002/14651858.CD009526.pub2. Cochrane Database Syst Rev. 2017. PMID: 29125183 Free PMC article.
-
Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: a systematic review and meta-analysis.Hum Reprod Update. 2014 Sep-Oct;20(5):748-58. doi: 10.1093/humupd/dmu012. Epub 2014 Mar 30. Hum Reprod Update. 2014. PMID: 24688118 Free PMC article.
-
Selenium supplementation for Hashimoto's thyroiditis.Cochrane Database Syst Rev. 2013 Jun 6;2013(6):CD010223. doi: 10.1002/14651858.CD010223.pub2. Cochrane Database Syst Rev. 2013. PMID: 23744563 Free PMC article.
-
Uterine morphology and anomalies in women with and without polycystic ovary syndrome: a systematic review and meta-analysis.Hum Reprod. 2025 Jun 19:deaf117. doi: 10.1093/humrep/deaf117. Online ahead of print. Hum Reprod. 2025. PMID: 40578330
References
-
- Liu Q., Tang B., Zhu Z., Kraft P., Deng Q., Stener-Victorin E., Jiang X. A genome-wide cross-trait analysis identifies shared loci and causal relationships of type 2 diabetes and glycaemic traits with polycystic ovary syndrome. Diabetologia. 2022;65:1483–1494. doi: 10.1007/s00125-022-05746-x. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
