

Chronic Low Back Pain in Young Adults: Pathophysiological Aspects of Neuroinflammation and Degeneration
- PMID: 40806719
- PMCID: PMC12347870
- DOI: 10.3390/ijms26157592
Chronic Low Back Pain in Young Adults: Pathophysiological Aspects of Neuroinflammation and Degeneration
Abstract
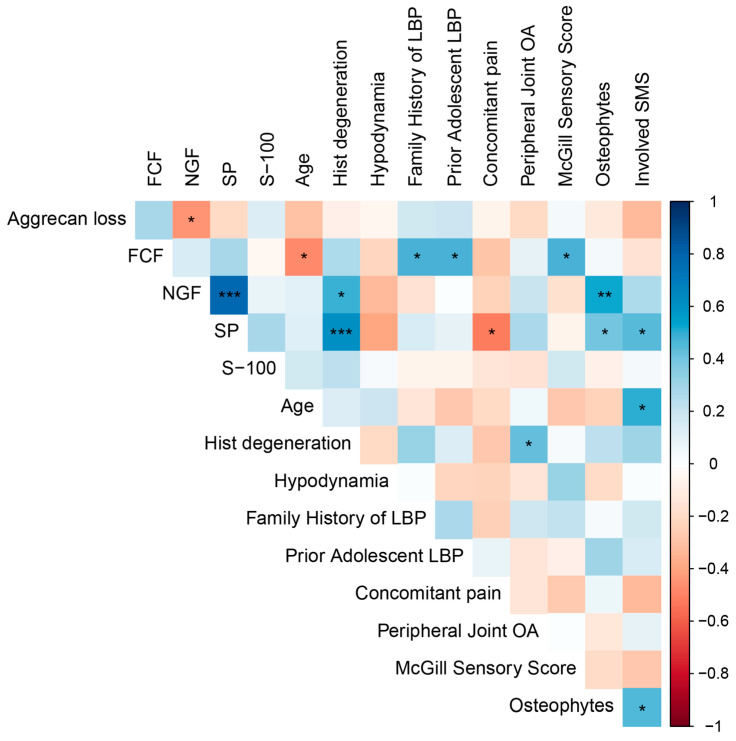
Degenerative disc disease (DDD) is a major cause of chronic low back pain (LBP), yet the molecular mechanisms driving disc degeneration and pain remain poorly understood. This study analyzed intervertebral disc (IVD) tissue from 36 young patients (median age = 36.00 [31.00, 42.50] years) with herniated discs and LBP, alongside healthy controls, to investigate changes in the extracellular matrix (ECM) and neurochemical alterations. Disc degeneration was assessed using MRI (Pfirrmann grading) and histology (Sive's criteria). Histochemical and immunohistochemical methods were used to evaluate aggrecan content, calcification, and the expression of nerve growth factor (NGF), substance P (SP), and S-100 protein. MRI findings included Pfirrmann grades V (30.55%), IV (61.11%), III (5.56%), and II (2.78%). Severe histological degeneration (10-12 points) was observed in three patients. Aggrecan depletion correlated with longer pain duration (r = 0.449, p = 0.031). NGF expression was significantly elevated in degenerated discs (p = 0.0287) and strongly correlated with SP (r = 0.785, p = 5.268 × 10-9). Free nerve endings were identified in 5 cases. ECM calcification, present in 36.1% of patients, was significantly associated with radiculopathy (r = 0.664, p = 0.005). The observed co-localization of NGF and SP suggests a synergistic role in pain development. These results indicate that in young individuals, aggrecan loss, neurochemical imbalance, and ECM calcification are key contributors to DDD and chronic LBP.
Keywords: NGF; S-100; aggrecan; back pain; calcification; degenerative disc disease; immunohistochemistry; substance P; young age.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures




Similar articles
-
The "horizon gray band" represents normal nucleus pulposus cells condense rather than intervertebral disc degeneration signal.Int J Surg. 2025 Jul 1;111(7):4339-4353. doi: 10.1097/JS9.0000000000002532. Epub 2025 May 26. Int J Surg. 2025. PMID: 40422293
-
Risk factors for progression of nucleus pulposus degeneration in the lumbar intervertebral disc: a retrospective analysis using the disc signal intensity index.Spine J. 2025 Jul;25(7):1466-1473. doi: 10.1016/j.spinee.2025.01.036. Epub 2025 Feb 1. Spine J. 2025. PMID: 39900250
-
Therapeutic effects of PDGF-AB/BB against cellular senescence in human intervertebral disc.Elife. 2025 Jul 16;13:RP103073. doi: 10.7554/eLife.103073. Elife. 2025. PMID: 40668091 Free PMC article.
-
Total disc replacement for chronic back pain in the presence of disc degeneration.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD008326. doi: 10.1002/14651858.CD008326.pub2. Cochrane Database Syst Rev. 2012. PMID: 22972118
-
The relationships between low back pain and lumbar lordosis: a systematic review and meta-analysis.Spine J. 2017 Aug;17(8):1180-1191. doi: 10.1016/j.spinee.2017.04.034. Epub 2017 May 2. Spine J. 2017. PMID: 28476690
References
-
- Russo F., Papalia G.F., Diaz Balzani L.A., Stelitano G., Zampogna B., Fontana L., Vadalà G., Iavicoli S., Papalia R., Denaro V. Prognostic Factors for Return to Work in Patients Affected by Chronic Low Back Pain: A Systematic Review. Musculoskelet. Surg. 2024;108:403–415. doi: 10.1007/s12306-024-00828-y. - DOI - PMC - PubMed
-
- Ferreira M.L., De Luca K., Haile L.M., Steinmetz J.D., Culbreth G.T., Cross M., Kopec J.A., Ferreira P.H., Blyth F.M., Buchbinder R., et al. Global, Regional, and National Burden of Low Back Pain, 1990–2020, Its Attributable Risk Factors, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5:e316–e329. doi: 10.1016/S2665-9913(23)00098-X. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
