

Sex Differences and Long-Term Outcomes in Patients with Left Bundle Branch Area Pacing Compared with Right Ventricular Pacing
- PMID: 40806879
- PMCID: PMC12347622
- DOI: 10.3390/jcm14155256
Sex Differences and Long-Term Outcomes in Patients with Left Bundle Branch Area Pacing Compared with Right Ventricular Pacing
Abstract
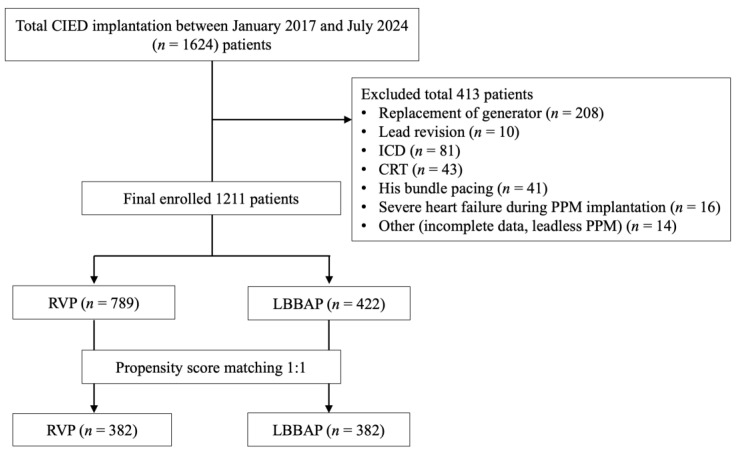
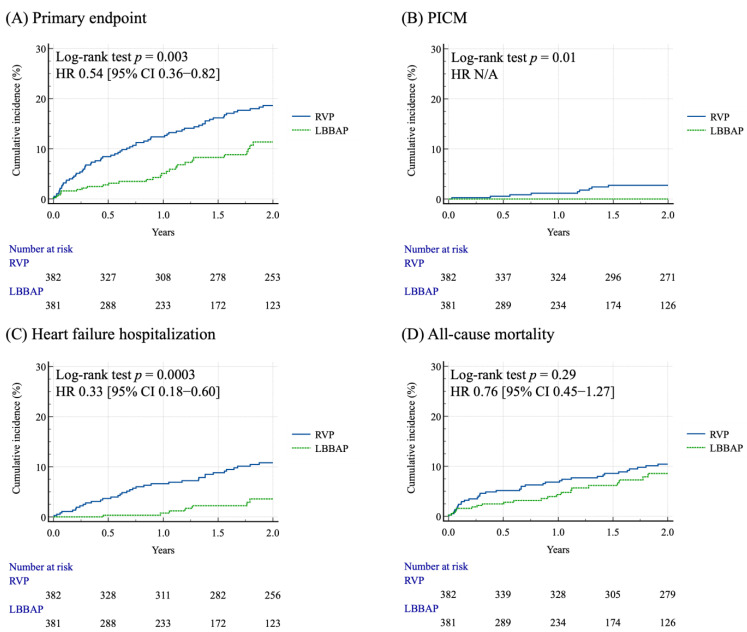
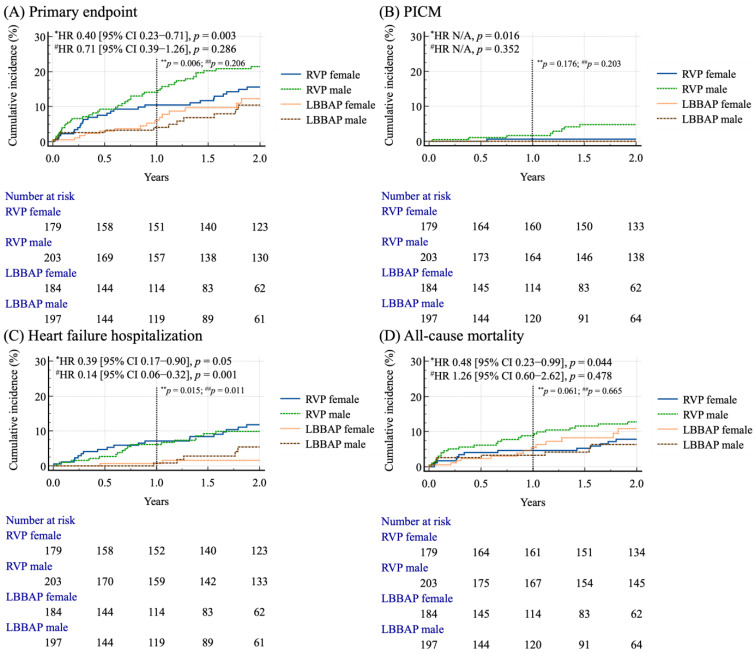
Background: Long-term right ventricular pacing (RVP) can cause electrical and mechanical dyssynchrony, resulting in adverse outcomes. Recently, left bundle branch area pacing (LBBAP) has emerged as a physiological pacing modality and is considered a promising alternative. To date, the long-term outcomes of LBBAP compared with RVP, particularly with respect to sex differences, remain unclear. Methods: Between January 2017 and July 2024, 1211 patients who underwent de novo pacemaker implantation were enrolled and categorized into RVP (n = 789) and LBBAP (n = 422). The primary outcome was a composite of all-cause mortality, heart failure hospitalization (HFH), and pacing-induced cardiomyopathy (PICM). Propensity score matching (PSM) was employed to minimize the selection bias and achieve comparability among the study population. A post hoc power analysis based on the observed effect size and sample size showed a power of 80%, confirming sufficient sensitivity to detect group differences. Results: After PSM, 764 patients were analyzed. The mean age of the patients was 74.6 ± 10.5 years in RVP and 74.5 ± 9.8 years in LBBAP, respectively, and 52.3% patients were male. Patients with LBBAP had a lower incidence of the primary outcome (8.6% vs. 24.6%, p < 0.001), HFH (2.6% vs. 13.6%, p < 0.001), and all-cause mortality (6.5% vs. 13.9%, p < 0.001) compared with RVP. There were no significant differences in the clinical outcomes, including the primary outcome, HFH and all-cause mortality, between the sexes in the group with either RVP or LBBAP. However, during a 2-year follow-up period for survival analysis, male patients with LBBAP had a significant lower incidence of all the endpoints, whereas female patients with LBBAP had a lower incidence of HFH [HR 0.14 (95% CI 0.06-0.32), p = 0.001] compared with those with RVP. Conclusions: Regardless of sex, patients with LBBAP had a lower risk of poor clinical outcomes, including HFH and all-cause mortality, compared to those with RVP. Moreover, compared with RVP, LBBAP decreased the risks of all the major endpoints in male patients and the risk of HFH particularly in female patients. Further research is needed to establish the sex-specific responses to LBBAP.
Keywords: clinical outcomes; heart failure hospitalization; left bundle branch area pacing; mortality; sex.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
