

EVAR Trends over the Past Decade and Their Impact on Aneurysm Mortality: National Health Insurance Data Analysis
- PMID: 40806898
- PMCID: PMC12347518
- DOI: 10.3390/jcm14155277
EVAR Trends over the Past Decade and Their Impact on Aneurysm Mortality: National Health Insurance Data Analysis
Abstract
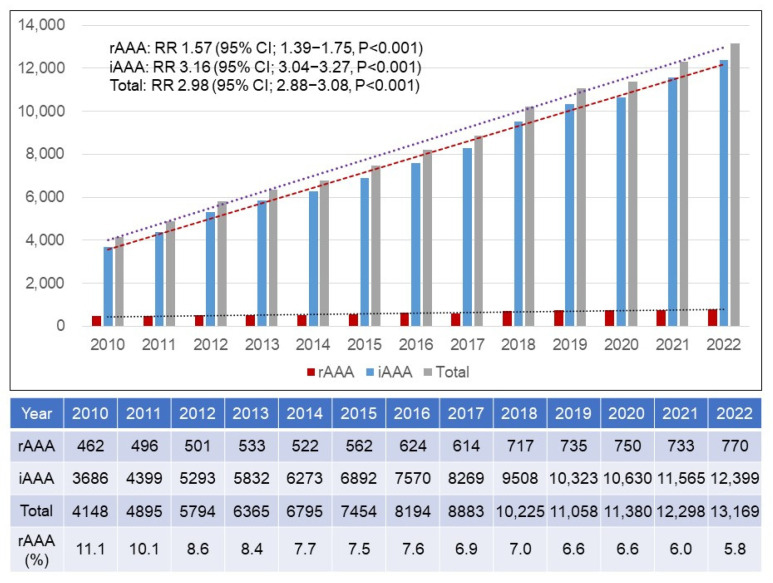
Background/Objectives: There are no reports about the nationwide trends in abdominal aortic aneurysm (AAA) repair and mortality rates. This study aims to evaluate the trend in AAA treatment and related mortality, including ruptured AAAs (rAAAs) and intact AAAs (iAAAs) over the last 13 years. Methods: This serial, cross-sectional study investigated the time trends in patients who were treated for an AAA and underwent an aneurysm repair between 2010 and 2022. Data from the Health Insurance Review and Assessment Service (HIRA) and Statistics Korea were used. A linear-by-linear association and Poisson regression analysis were performed to determine the changes in the treatment of AAAs and related mortality. Results: The number of patients with an rAAA increased from 462 in 2010 to 770 in 2022 (relative risk, RR 1.57; p < 0.0001). The number of patients with an iAAA increased from 3685 to 12,399 in the same period (RR 3.16; p < 0.0001). Endovascular aneurysm repair (EVAR) has been more commonly performed since 2011. During the study period, EVAR increased from 406 to 1161 (RR 2.68; p < 0.0001). Although the annual mortality rates after iAAA treatment decreased from 1.4% to 0.7% (mean mortality rate, 1.1%), the mortality rates after rAAA treatment were similar, ranging from 34.6% to 34.2%, during the study period (mean mortality rate, 35.2%). Conclusions: During the last 13 years, the annual number of patients with rAAAs and iAAAs has increased. Since 2011, EVAR has been more commonly performed. The annual iAAA-related mortality rate decreased along with the increasing trend in EVAR. However, the annual rAAA-related mortality rate did not change.
Keywords: abdominal; aortic aneurysm; endovascular aneurysm repair; mortality; open abdomen techniques.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




Similar articles
-
Endovascular treatment for ruptured abdominal aortic aneurysm.Cochrane Database Syst Rev. 2014 Jul 21;(7):CD005261. doi: 10.1002/14651858.CD005261.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2017 May 26;5:CD005261. doi: 10.1002/14651858.CD005261.pub4. PMID: 25042123 Updated.
-
Endovascular treatment for ruptured abdominal aortic aneurysm.Cochrane Database Syst Rev. 2017 May 26;5(5):CD005261. doi: 10.1002/14651858.CD005261.pub4. Cochrane Database Syst Rev. 2017. PMID: 28548204 Free PMC article.
-
Laparoscopic surgery for elective abdominal aortic aneurysm repair.Cochrane Database Syst Rev. 2017 May 4;5(5):CD012302. doi: 10.1002/14651858.CD012302.pub2. Cochrane Database Syst Rev. 2017. PMID: 28471523 Free PMC article.
-
Endovascular repair of abdominal aortic aneurysm.Cochrane Database Syst Rev. 2014 Jan 23;2014(1):CD004178. doi: 10.1002/14651858.CD004178.pub2. Cochrane Database Syst Rev. 2014. PMID: 24453068 Free PMC article.
-
Totally percutaneous versus surgical cut-down femoral artery access for elective bifurcated abdominal endovascular aneurysm repair.Cochrane Database Syst Rev. 2023 Jan 11;1(1):CD010185. doi: 10.1002/14651858.CD010185.pub4. Cochrane Database Syst Rev. 2023. PMID: 36629152 Free PMC article.
References
-
- Greenhalgh R.M., Brown L.C., Kwong G.P., Powell J.T., Thompson S.G., EVAR trial participants Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: Randomised controlled trial. Lancet. 2004;364:843–848. doi: 10.1016/S0140-6736(04)16979-1. - DOI - PubMed
-
- Prinssen M., Verhoeven E.L., Buth J., Cuypers P.W., van Sambeek M.R., Balm R., Buskens E., Grobbee D.E., Blankensteijn J.D., Dutch Randomized Endovascular Aneurysm Management (DREAM) Trial Group A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N. Engl. J. Med. 2004;351:1607–1618. doi: 10.1056/NEJMoa042002. - DOI - PubMed
-
- Lederle F.A., Freischlag J.A., Kyriakides T.C., Padberg F.T., Jr., Matsumura J.S., Kohler T.R., Lin P.H., Jean-Claude J.M., Cikrit D.F., Swanson K.M., et al. Outcomes following endovascular vs open repair of abdominal aortic aneurysm: A randomized trial. JAMA. 2009;302:1535–1542. doi: 10.1001/jama.2009.1426. - DOI - PubMed
-
- Chaikof E.L., Dalman R.L., Eskandari M.K., Jackson B.M., Lee W.A., Mansour M.A., Mastracci T.M., Mell M., Murad M.H., Nguyen L.L., et al. Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. J. Vasc. Surg. 2018;67:2–77. doi: 10.1016/j.jvs.2017.10.044. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
