

SGLT2 Inhibitors and the Risk of Arrhythmias in Heart Failure: A Network Meta-Analysis
- PMID: 40806928
- PMCID: PMC12347573
- DOI: 10.3390/jcm14155306
SGLT2 Inhibitors and the Risk of Arrhythmias in Heart Failure: A Network Meta-Analysis
Abstract
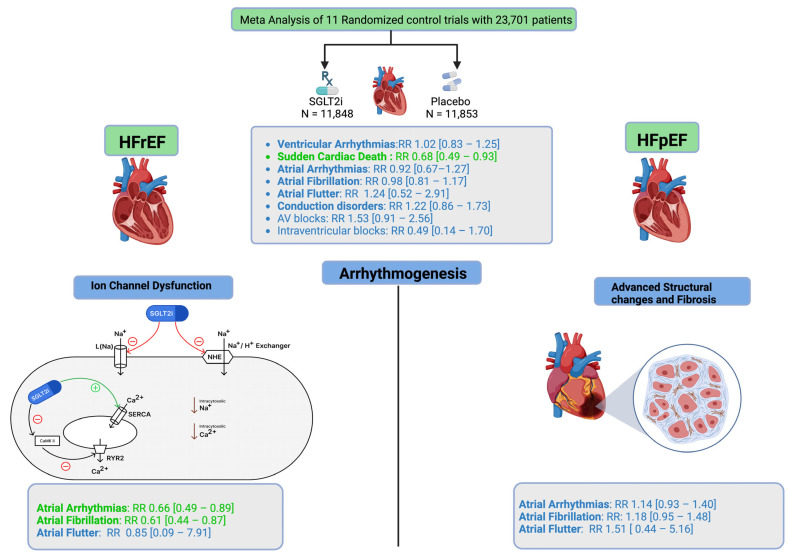
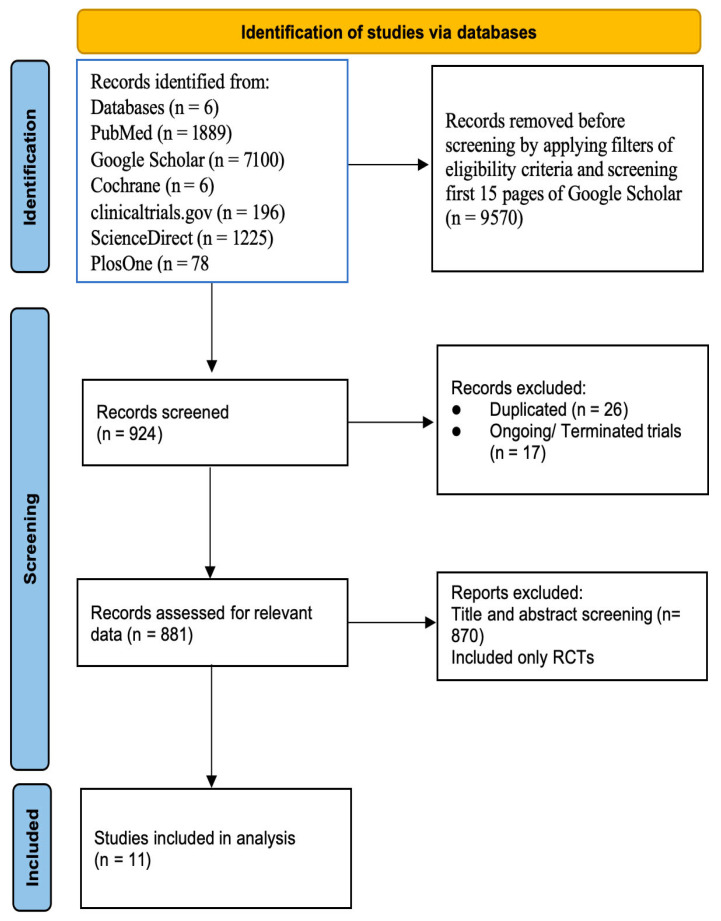
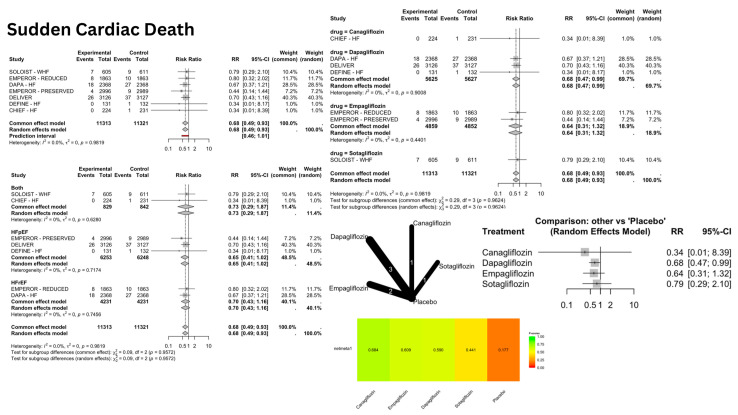
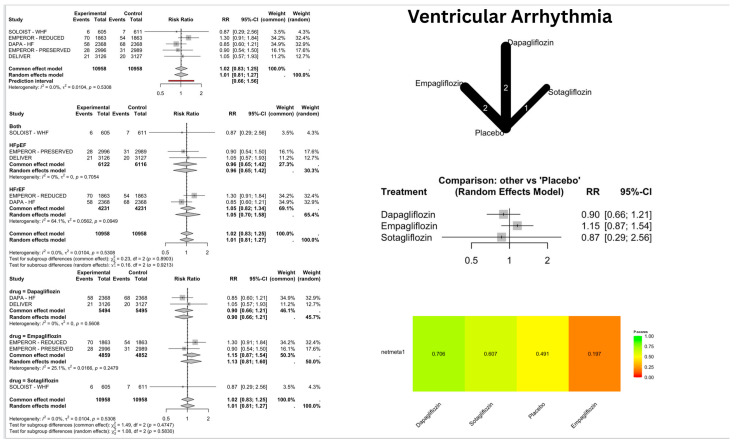
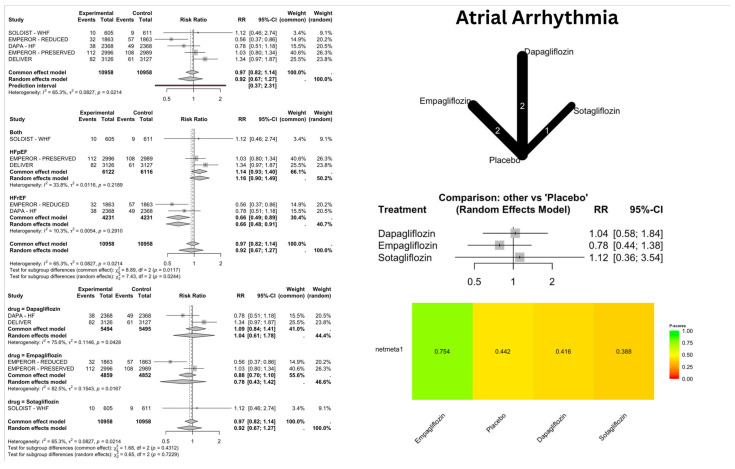
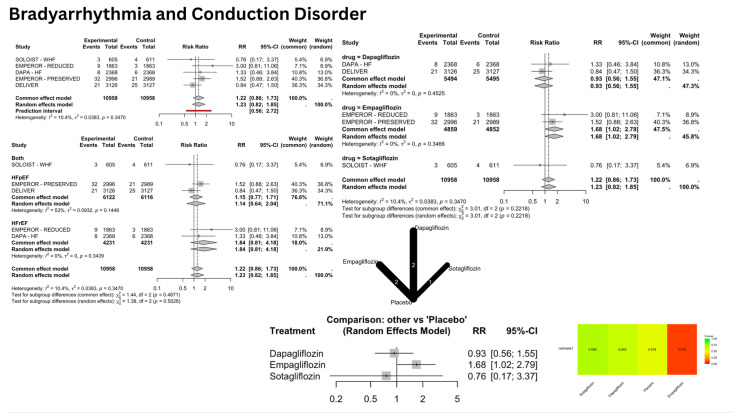
Background/Objectives: Sodium-glucose cotransporter-2 inhibitors (SGLT2i) have revolutionized heart failure (HF) therapies and are an essential component of guideline-directed medical therapy (GDMT); however, their significance in arrhythmia prevention is still uncertain. This meta-analysis evaluates the benefits of SGLT2i on arrhythmias in HF. Methods: A comprehensive examination was performed with PubMed, ScienceDirect, PLOS One, Cochrane, Google Scholar, and ClinicalTrials.gov from January 2014 to March 2025, complying with PRISMA guidelines. Randomized controlled trials (RCTs) comparing SGLT2i with placebo were incorporated. Primary results included ventricular arrhythmias (VA), sudden cardiac death (SCD), atrial arrhythmias, and conduction disorders. Subgroup analyses investigated the effects on arrhythmias in HF with reduced ejection fraction (HFrEF) and preserved ejection fraction (HFpEF). Results: A total of 11 RCTs involving 23,701 patients, 11,848 on SGLT2i (mean age: 68.26 ± 10 yrs, 53.5% males) and 11,853 on placebo (mean age: 67.91 ± 10 yrs, 53% males), were analyzed with a mean follow-up of 2.71 yrs. No significant differences were reported between SGLT2i and placebo for VA [relative risk (RR): 1.02, 95% confidence interval (CI): 0.83-1.25], I2 =0%), atrial arrhythmias (RR: 0.92 [CI: 0.67-1.27], I2 = 65.3%), or conduction disorders (RR:1.22 [CI: 0.86-1.73], I2 = 10.4%). Notably, significant reductions in risk of SCD (RR: 0.68 [CI: 0.49-0.93], I2 = 0%) and in the risk of atrial arrhythmias in HFrEF (RR: 0.66 [CI: 0.49-0.89], I2 = 10.3%) were witnessed, although no such reduction was seen in HFpEF (RR: 1.14 [CI: 0.94-1.40], I2 = 33.8%). Conclusions: SGLT2i do not reduce overall arrhythmia or conduction disorder risk in HF but significantly reduce the risk of SCD and atrial arrhythmias in HFrEF patients. These results highlight potential arrhythmia prevention benefits in HFrEF, warranting further targeted studies.
Keywords: arrhythmia; atrial fibrillation; sodium-glucose cotransporter-2 inhibitor; sudden cardiac death.
Conflict of interest statement
Fonarow reports consulting for Abbott Amgen, AstraZeneca Bayer, Boehinger Ingelheim, Cytokinetics, Eli Lilly, Johnson & Johnson, Medtronic Merck, Novartis and Pfizer. The other authors have nothing to disclose.
Figures
Similar articles
-
The cardiovascular effects of SGLT2 inhibitors, RAS inhibitors, and ARN inhibitors in heart failure.ESC Heart Fail. 2023 Apr;10(2):1314-1325. doi: 10.1002/ehf2.14298. Epub 2023 Feb 1. ESC Heart Fail. 2023. PMID: 36722326 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Exercise-based rehabilitation for heart failure.Cochrane Database Syst Rev. 2014 Apr 27;2014(4):CD003331. doi: 10.1002/14651858.CD003331.pub4. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2019 Jan 29;1:CD003331. doi: 10.1002/14651858.CD003331.pub5. PMID: 24771460 Free PMC article. Updated.
-
Association between sodium-glucose cotransporter-2 inhibitors and incident atrial fibrillation/atrial flutter in heart failure patients with reduced ejection fraction: a meta-analysis of randomized controlled trials.Heart Fail Rev. 2023 Jul;28(4):925-936. doi: 10.1007/s10741-022-10281-3. Epub 2022 Oct 25. Heart Fail Rev. 2023. PMID: 36282460 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
References
-
- World Heart Federation Heart Failure. [(accessed on 25 June 2025)]. Available online: https://world-heart-federation.org/what-we-do/heart-failure/
-
- Bozkurt B., Ahmad T., Alexander K.M., Baker W.L., Bosak K., Breathett K., Fonarow G.C., Heidenreich P., Ho J.E., Hsich E., et al. Heart failure epidemiology and outcomes statistics: A report of the Heart Failure Society of America. J. Card. Fail. 2023;29:1412–1451. doi: 10.1016/j.cardfail.2023.07.006. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
