

Obesity Is a Thrombotic Risk Factor in Pregnant Women
- PMID: 40806932
- PMCID: PMC12347431
- DOI: 10.3390/jcm14155310
Obesity Is a Thrombotic Risk Factor in Pregnant Women
Abstract
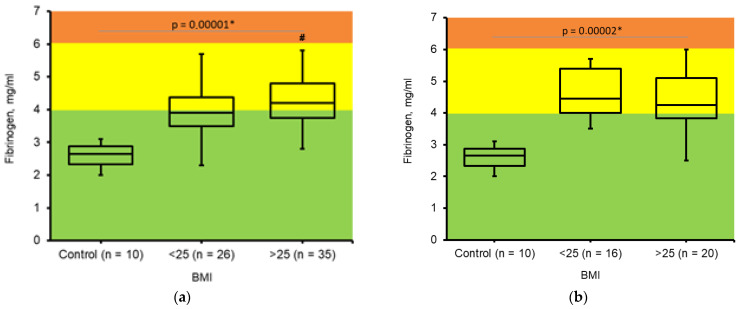
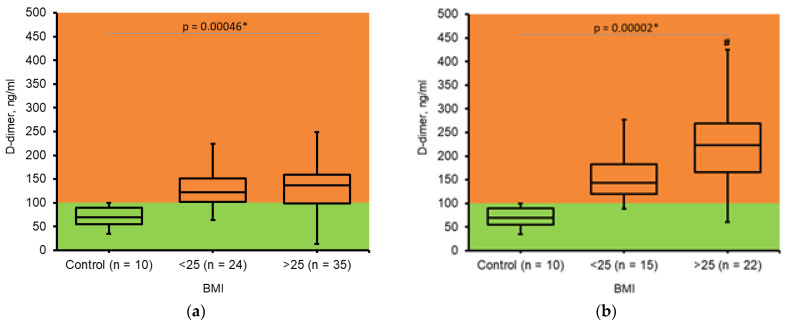
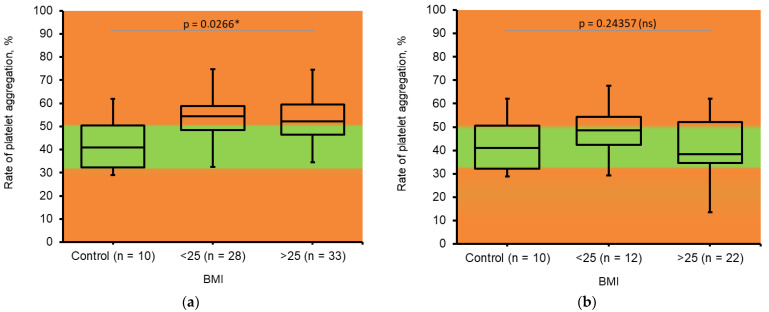
Background/Objectives: Pregnancy is associated with increased procoagulant conditions, and when combined with obesity, it can elevate the risk of thrombosis. The study aims to assess thrombosis risk markers during pregnancy in relation to obesity. Methods: Somatically healthy women aged 18-42 years with spontaneous pregnancies who did not receive specific antithrombotic treatment were enrolled in the study (n = 97). The participants were divided into groups based on pregestational BMI: the first group consisted of patients who had a BMI ≤ 25 (n = 42), and the second group consisted of patients who were overweight (BMI > 25) and obese (BMI > 30) (n = 55). The control group comprised healthy, non-pregnant, non-obese women (n = 10). Results: Fibrinogen levels, elevated during pregnancy, were higher in the II and III trimesters, with gestational period having a greater influence than BMI. Moderate D-dimer accumulation was observed regardless of obesity, but higher levels were seen in obese women during the III trimester, indicating the dissolution of intravascular fibrin deposits. Soluble fibrin was significantly higher in obese and overweight women during the II trimester and elevated in both groups during the III trimester, correlating with D-dimer accumulation and indicating thrombus formation. A decrease in platelet aggregation ability was observed correlating with D-dimer and soluble fibrin patterns. Conclusions: A significant accumulation of thrombosis risk markers was observed in the III trimester compared to the II, occurring earlier in obese and overweight pregnant women and indicating a higher risk of thrombotic complications in obesity.
Keywords: D-dimer; fibrinogen; obesity; platelets; pregnancy; soluble fibrin; thrombosis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Fatokun T.B., Swartz S.E., Ebeid A., Cordes S.A., Gimovsky A.C., Sparks A.D., Amdur R.L., Ahmadzia H.K. Venous Thromboembolism Risk Factors in Women with Obesity Who Undergo Cesarean Delivery. Clin. Appl. Thromb. Hemost. 2024;30:10760296241247203. doi: 10.1177/10760296241247203. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
