

Implant-Supported Oral Rehabilitation in Head and Neck Cancer Patients: A 20-Year Single-Center Study (2005-2024)
- PMID: 40807055
- PMCID: PMC12347589
- DOI: 10.3390/jcm14155435
Implant-Supported Oral Rehabilitation in Head and Neck Cancer Patients: A 20-Year Single-Center Study (2005-2024)
Abstract
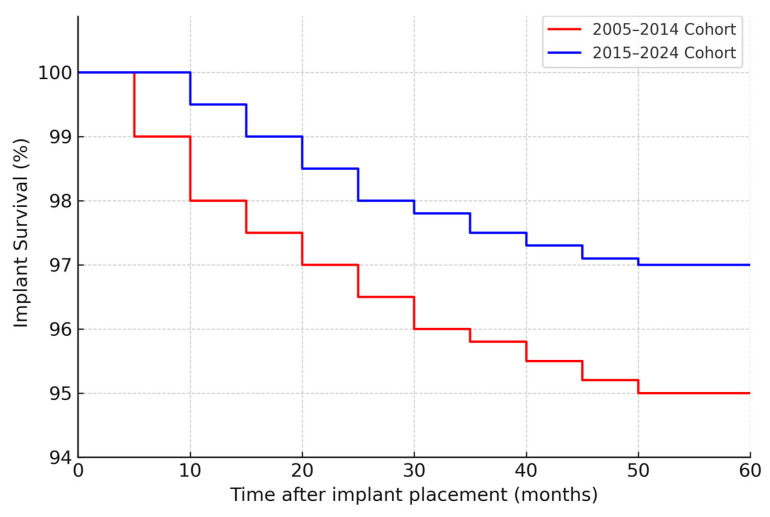
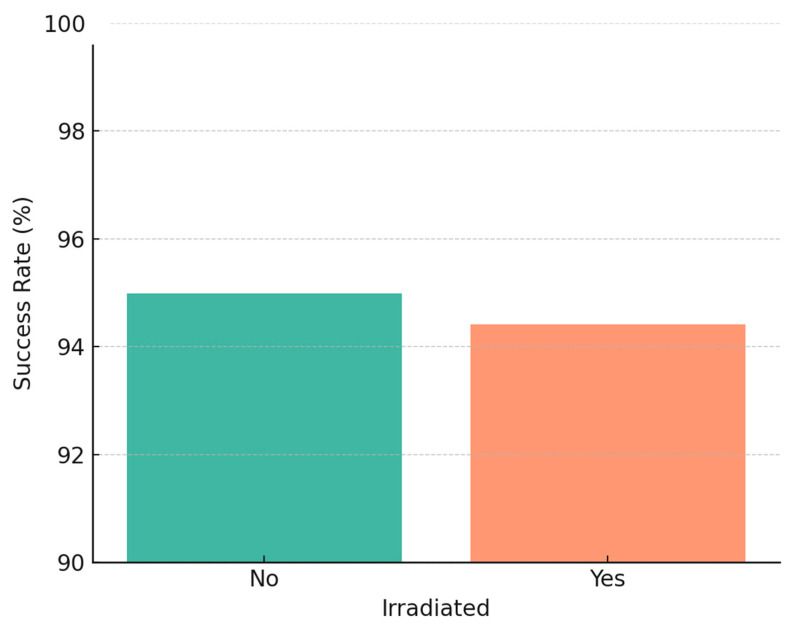
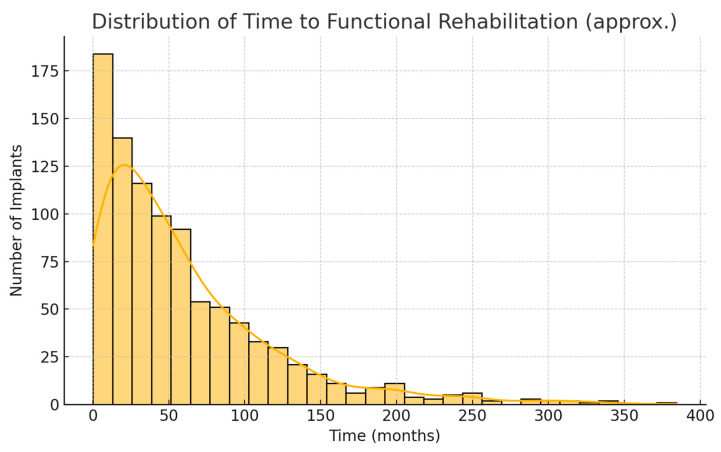
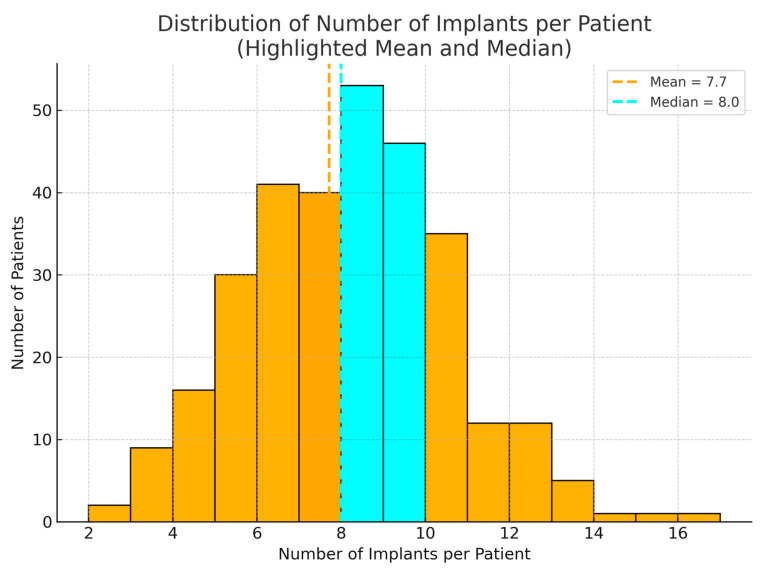
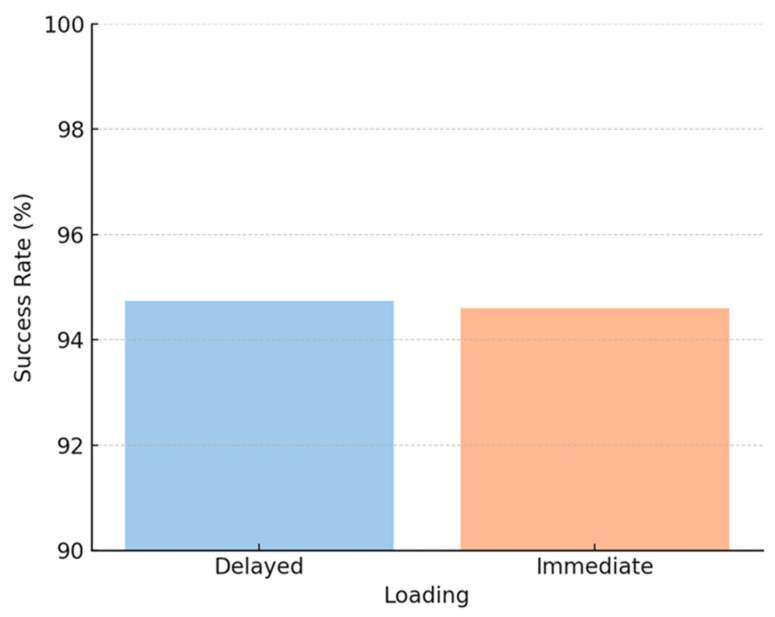
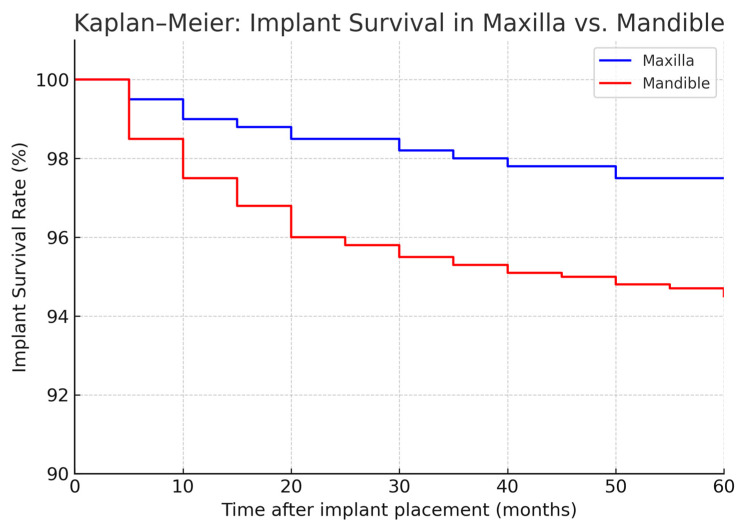
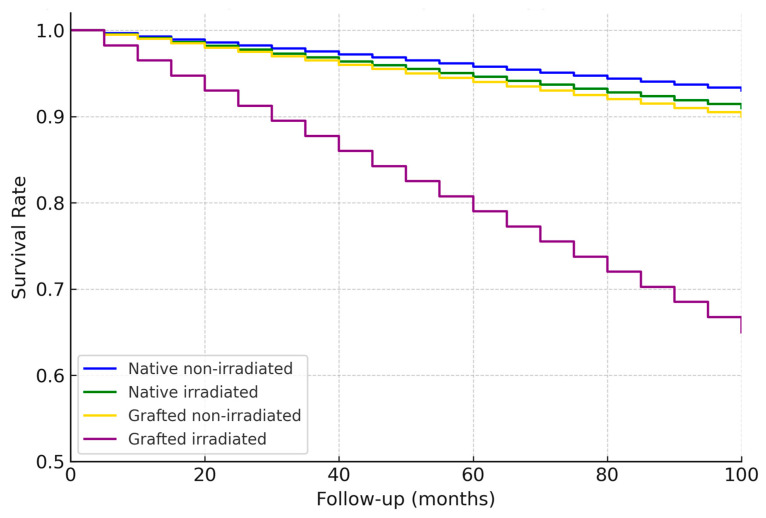
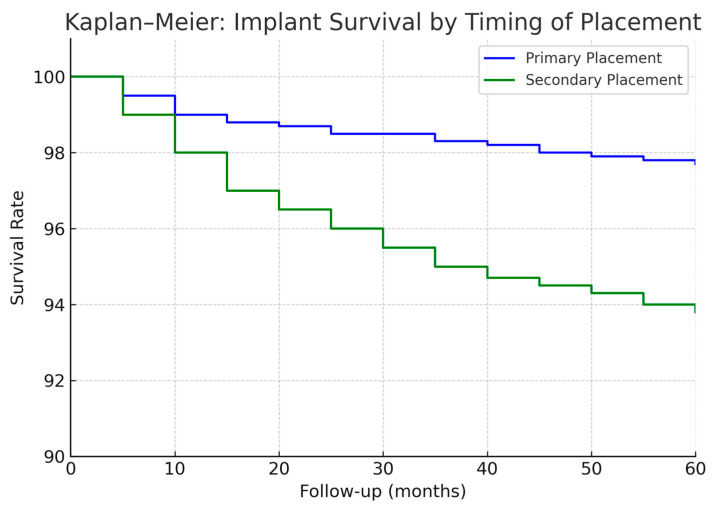
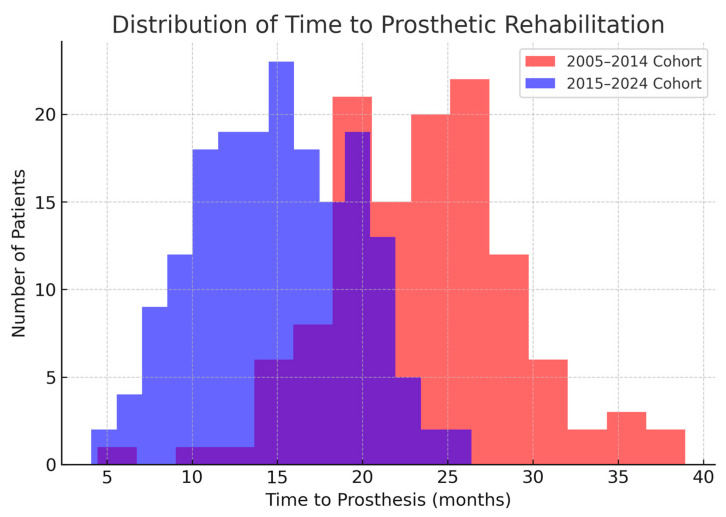
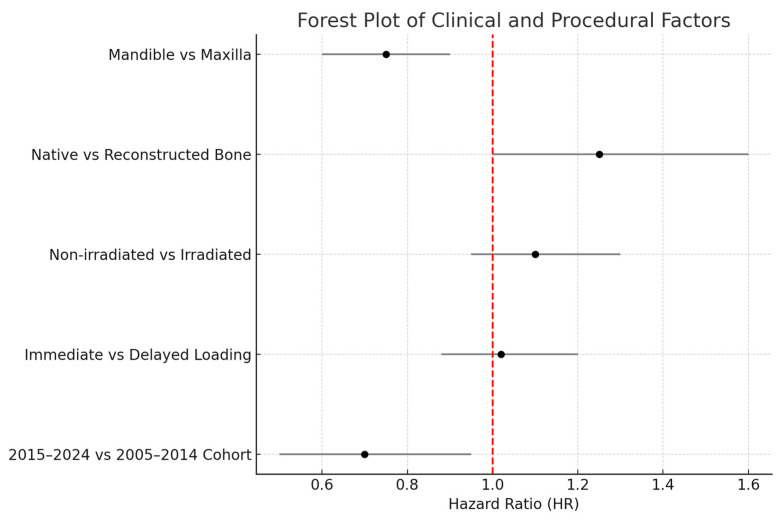
Background/Objectives: Oral cancer resection often leads to maxillofacial defects and dentition loss, compromising patients' quality of life. Implant-supported prosthetic rehabilitation offers a reliable solution to restore function, though factors such as bone reconstruction, radiotherapy, and timing of implant placement (immediate vs. delayed) may influence outcomes. This study aimed to evaluate long-term implant survival and rehabilitation timelines in oncologic patients, comparing two cohorts (2005-2014 and 2015-2024) to assess the impact of evolving clinical practices. Methods: A retrospective cohort study was conducted at Hospital General Universitario Gregorio Marañón (Madrid, Spain), including 304 patients who underwent ablative oral cancer surgery and subsequent implant-based rehabilitation between 2005 and 2024. Data on demographics, oncologic treatment, reconstruction, implant timing, and prosthetic rehabilitation were collected. Outcomes were compared using Kaplan-Meier analysis and appropriate statistical tests between the 2005-2014 (n = 122) and 2015-2024 (n = 182) cohorts. Results: A total of 2341 Ticare Implants® were placed, supporting 281 prostheses. Implant placement during primary surgery increased from 41% to 71% (p < 0.001). The median time from surgery to prosthesis significantly decreased from 24 to 15 months (p < 0.001). Five-year implant survival was 95% in the early cohort versus 97% in the later cohort. Implant survival was comparable between irradiated and non-irradiated patients (~94-96%). Fixed prostheses became more frequent (92% vs. 79%, p = 0.002). Conclusions: Implant-supported rehabilitation in oncologic patients is highly feasible and durable, with improved timelines and functional outcomes associated with early implant placement and modern digital planning strategies.
Keywords: 3D printing; dental implants; free fibula flap; head and neck oncology; implant stability quotient; implant survival; oral cancer; osseointegration; point-of-care manufacturing; prosthetic rehabilitation; radiotherapy.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures

Similar articles
-
Does Augmenting Irradiated Autografts With Free Vascularized Fibula Graft in Patients With Bone Loss From a Malignant Tumor Achieve Union, Function, and Complication Rate Comparably to Patients Without Bone Loss and Augmentation When Reconstructing Intercalary Resections in the Lower Extremity?Clin Orthop Relat Res. 2025 Jun 26. doi: 10.1097/CORR.0000000000003599. Online ahead of print. Clin Orthop Relat Res. 2025. PMID: 40569278
-
Interventions for replacing missing teeth: different times for loading dental implants.Cochrane Database Syst Rev. 2013 Mar 28;2013(3):CD003878. doi: 10.1002/14651858.CD003878.pub5. Cochrane Database Syst Rev. 2013. PMID: 23543525 Free PMC article.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus.Cochrane Database Syst Rev. 2014 May 13;2014(5):CD008397. doi: 10.1002/14651858.CD008397.pub2. Cochrane Database Syst Rev. 2014. PMID: 24825543 Free PMC article.
-
Does Transhumeral Osseointegration After Amputation Improve Patient-reported Outcomes and Prosthesis Use?Clin Orthop Relat Res. 2025 Feb 19;483(8):1502-1510. doi: 10.1097/CORR.0000000000003420. Clin Orthop Relat Res. 2025. PMID: 39982023
References
LinkOut - more resources
Full Text Sources
