

Updates in Contemporary Management of Singleton Pregnancies Complicated by a Short Cervix
- PMID: 40807162
- PMCID: PMC12347413
- DOI: 10.3390/jcm14155544
Updates in Contemporary Management of Singleton Pregnancies Complicated by a Short Cervix
Abstract
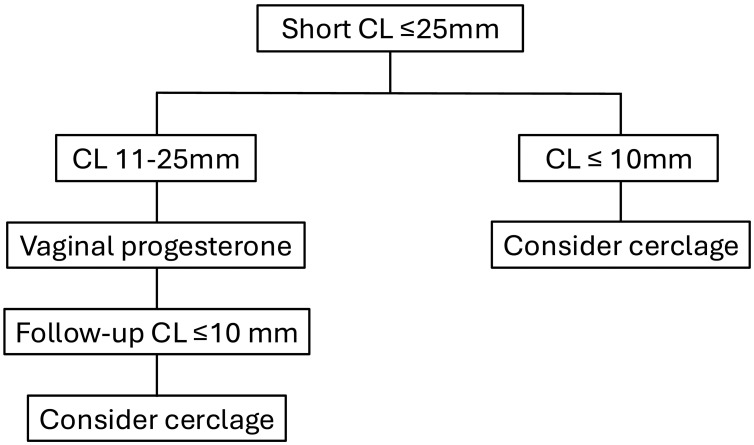
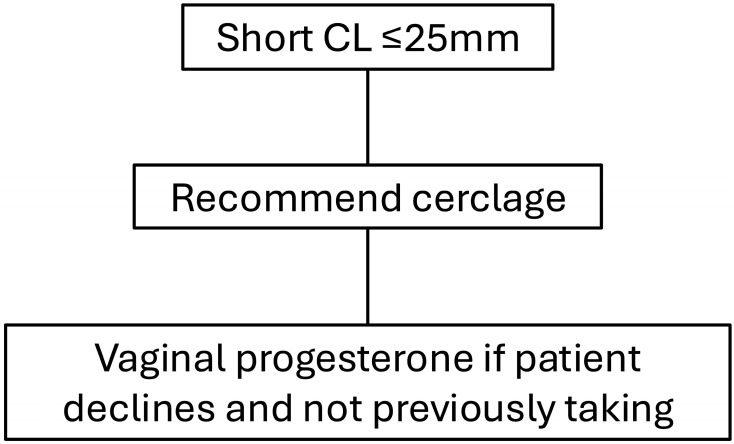
Singleton pregnancies complicated by a short cervical length (≤25 mm) are at significantly increased risk for spontaneous preterm birth. Several treatment strategies aimed at reducing this risk and improving perinatal outcomes have been evaluated, including vaginal progesterone, cervical cerclage, and cervical pessary. This review summarizes the latest evidence regarding the efficacy of these interventions. Vaginal progesterone and/or cervical cerclage have been identified as proven evidence-based practices for preterm birth prevention and improve neonatal outcomes. Vaginal progesterone reduces the risk of preterm birth < 35 weeks by 27% (relative risk 0.73, 95% confidence interval 0.58-0.90). Cervical cerclage has been shown to reduce the risk of preterm birth < 35 weeks by 30% (relative risk 0.70, 95% confidence interval 0.55-0.89) in patients with a short cervical length and prior preterm birth. In contrast, recent data suggest that cervical pessary should no longer be considered a management option for these patients. A continued focus on individualized, evidence-based approaches remains essential to optimizing outcomes in this high-risk population.
Keywords: cerclage; cervical length; cervical pessary; neonatal morbidity; prematurity; preterm birth; vaginal progesterone.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Cervical pessary for preventing preterm birth in singleton pregnancies.Cochrane Database Syst Rev. 2022 Dec 1;12(12):CD014508. doi: 10.1002/14651858.CD014508. Cochrane Database Syst Rev. 2022. PMID: 36453699 Free PMC article.
-
Cervical stitch (cerclage) for preventing preterm birth in singleton pregnancy.Cochrane Database Syst Rev. 2017 Jun 6;6(6):CD008991. doi: 10.1002/14651858.CD008991.pub3. Cochrane Database Syst Rev. 2017. PMID: 28586127 Free PMC article.
-
Interventions to prevent preterm birth following fetoscopic laser surgery for twin-to-twin transfusion syndrome: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2025 Jul;66(1):14-23. doi: 10.1002/uog.29230. Epub 2025 Jun 5. Ultrasound Obstet Gynecol. 2025. PMID: 40470767 Free PMC article. Review.
-
Interventions to prevent spontaneous preterm birth in women with singleton pregnancy who are at high risk: systematic review and network meta-analysis.BMJ. 2022 Feb 15;376:e064547. doi: 10.1136/bmj-2021-064547. BMJ. 2022. PMID: 35168930 Free PMC article.
-
Role of progesterone, cerclage and pessary in preventing preterm birth in twin pregnancies: A systematic review and network meta-analysis.Eur J Obstet Gynecol Reprod Biol. 2021 Jun;261:166-177. doi: 10.1016/j.ejogrb.2021.04.023. Epub 2021 Apr 24. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 33946019
References
Publication types
LinkOut - more resources
Full Text Sources
