

Demographics, risk factors associated with malignant progression, and pregnancy outcomes of hydatidiform mole: A retrospective cohort study in Shanghai, China
- PMID: 40809033
- PMCID: PMC12343242
- DOI: 10.3389/fonc.2025.1643590
Demographics, risk factors associated with malignant progression, and pregnancy outcomes of hydatidiform mole: A retrospective cohort study in Shanghai, China
Abstract
Objective: This study aimed to clarify the demographics, evaluate risk factors associated with malignant progression, and assess pregnancy outcomes among patients with hydatidiform mole (HM) using a large, retrospective cohort study in Shanghai.
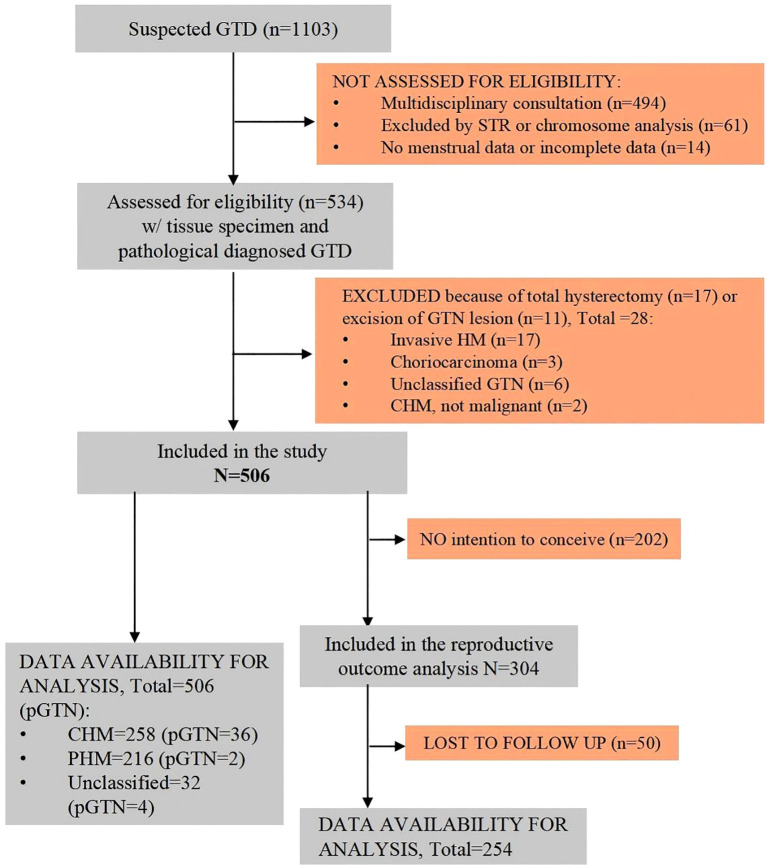
Methods: This retrospective cohort study included patients with pathologically confirmed HM from 2019 to 2023. Descriptive analyses were performed to describe the demographic characteristics, progression to postmolar gestational trophoblastic neoplasia (pGTN), and reproductive outcomes of patients. Univariate and multivariate logistic regression analyses were conducted to evaluate risk factors and develop predictive models for pGTN.
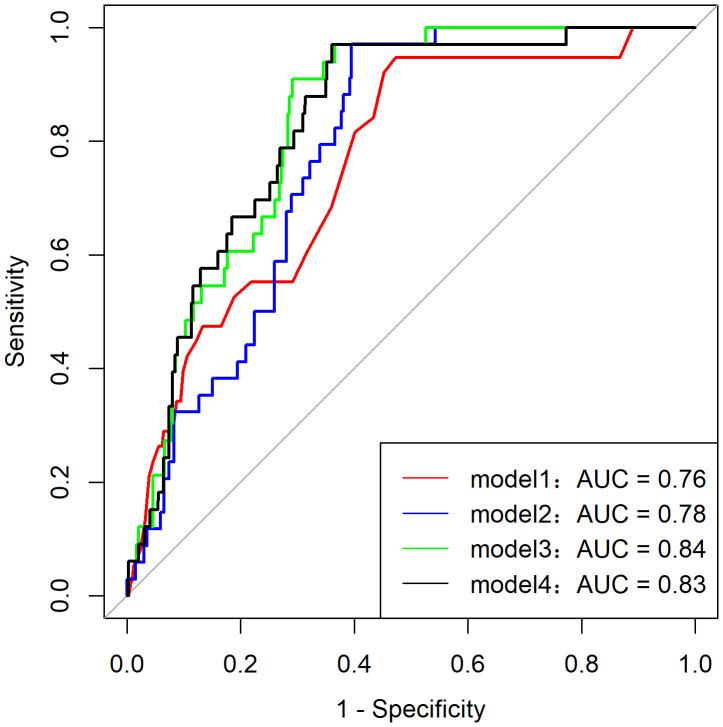
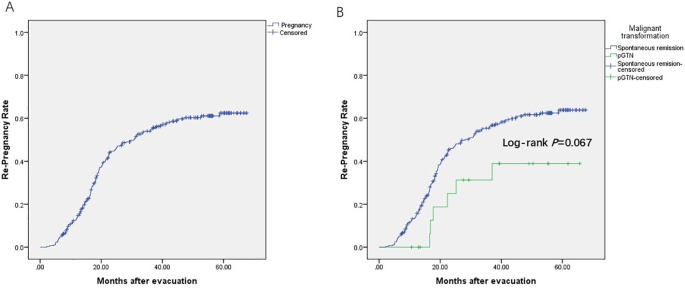
Results: Of 506 patients with HM, the average age and gestational age at diagnosis were approximately 33 years and 10 weeks, respectively. During follow-up, 42 patients (8.3%) progressed to pGTN, all achieved complete response after treatment. Univariate and multivariate analyses revealed that significant risk factors for progression to pGTN included pathological type and maximum diameter of lesions by ultrasound pre-evacuation (p < 0.05 for both). A predictive model incorporating age, β-hCG ratio (before/after evacuation), and ultrasound characteristics (uterine/lesion ratio) demonstrated optimal performance and goodness of fit. Among the 304 patients who intended to conceive, 254 had documented reproductive outcomes (follow-up rate: 83.6%). Of these, 163 patients (64.2%) achieved successful re-pregnancy, including 131 (80.4%) livebirths.
Conclusion: Our study provides a comprehensive update on the demographics, risk factors associated with progression to pGTN, and reproductive outcomes of patients with HM in Shanghai. The clinical application of the predictive model needs to be further verified in a longitudinal setting.
Keywords: demographics; hydatidiform mole; postmolar gestational trophoblastic neoplasia; pregnancy outcome; risk factor.
Copyright © 2025 Zhu, Zhu, Ma, Yu, Chen, Tao, Sun, Lu and Du.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
LinkOut - more resources
Full Text Sources