

Global pulmonary arterial hypertension trends and projections to 2046: a multi-method analysis of epidemiologic and demographic drivers using GBD 2021
- PMID: 40809197
- PMCID: PMC12340296
- DOI: 10.21037/jtd-2025-305
Global pulmonary arterial hypertension trends and projections to 2046: a multi-method analysis of epidemiologic and demographic drivers using GBD 2021
Abstract
Background: Pulmonary arterial hypertension (PAH) is a progressive disease that affects millions of individuals worldwide. This investigation predicted PAH burden pattern and temporal trends to provide epidemiologic evidence.
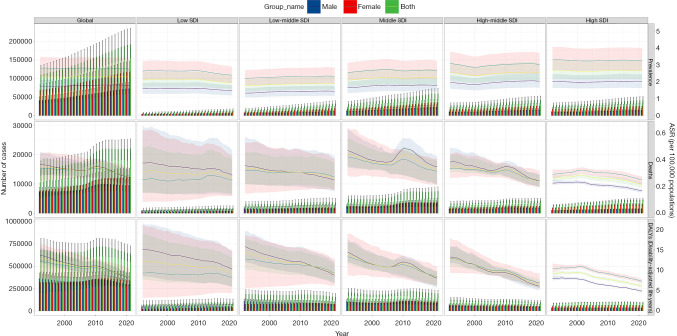
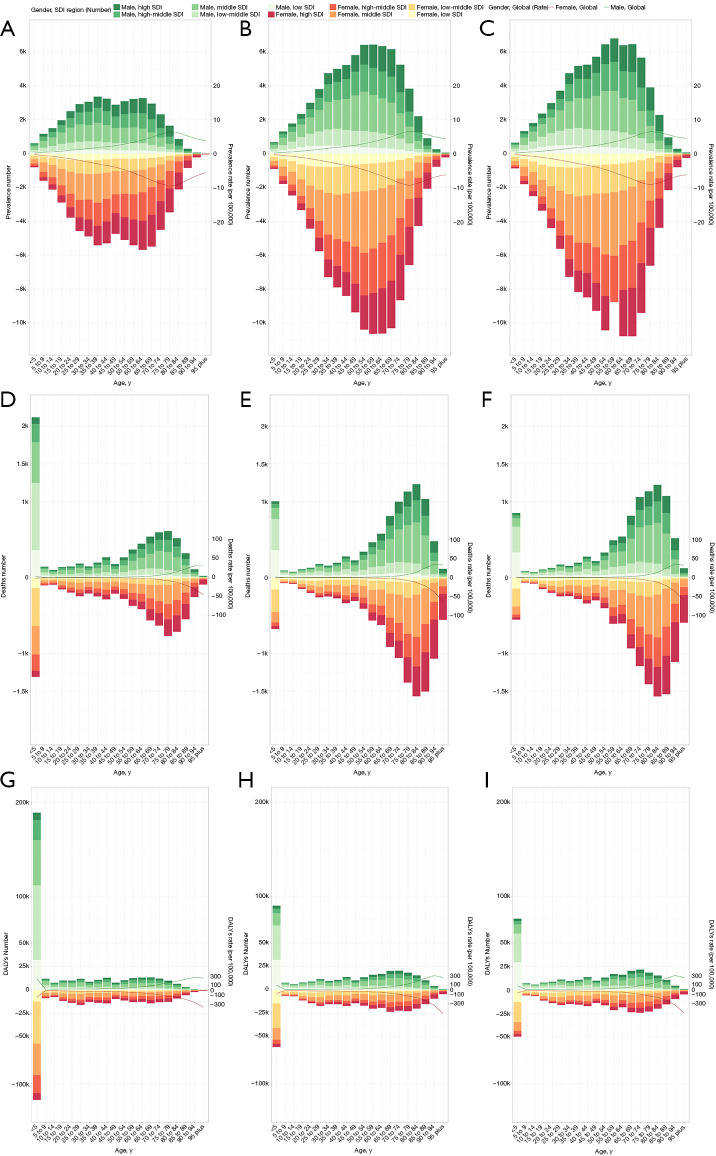
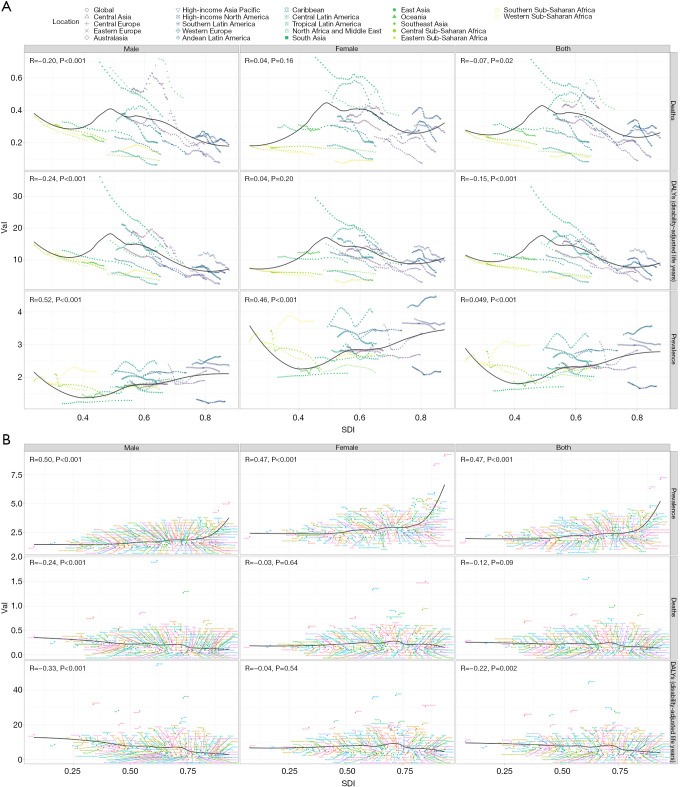
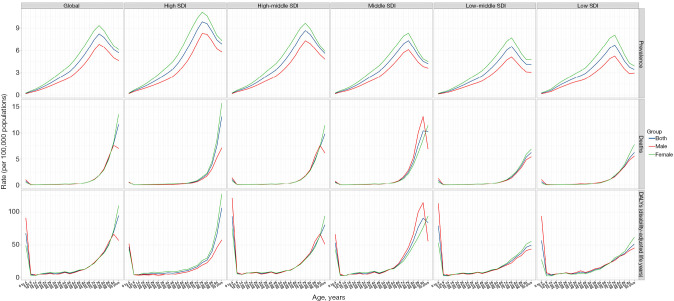
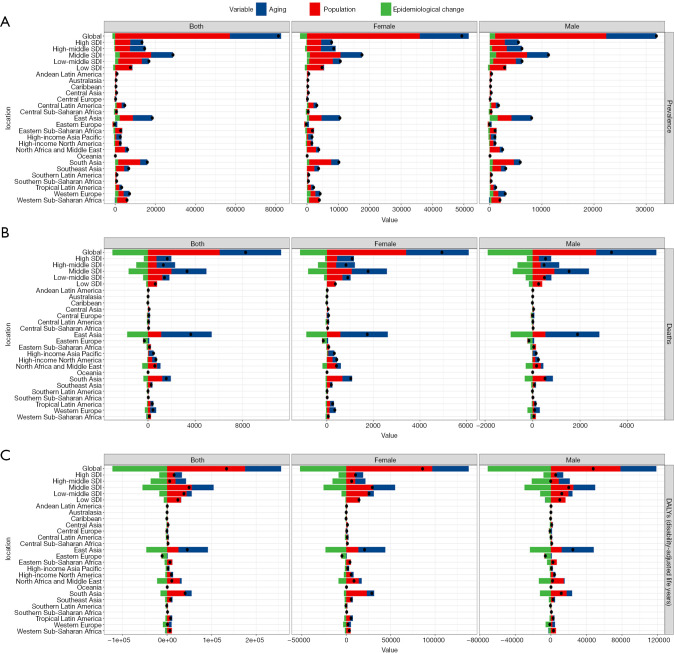
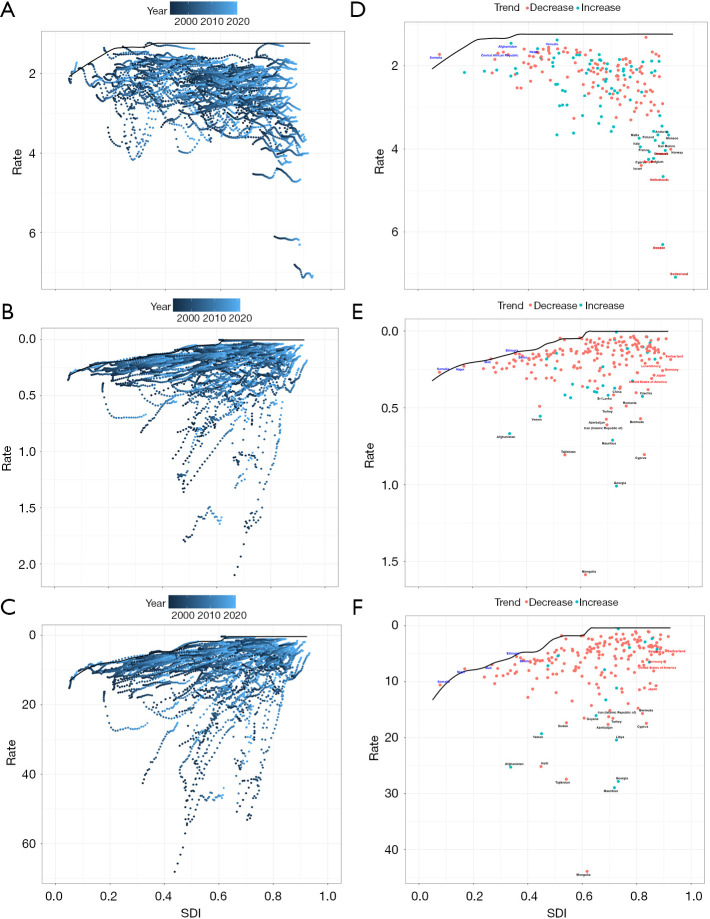
Methods: Data on prevalence, mortality and disability-adjusted life years (DALYs) was extracted from the Global Burden of Diseases (GBD) 2021. Subgroup analyses were performed based on sex, geographical regions, and socio-demographic index (SDI). Joinpoint model, Bayesian age-period-cohort (BAPC) model, age-period-cohort analysis, decomposition methodology and frontier analysis were employed to evaluate the temporal trends from 1992 to 2021, forecast the disease burden up to 2046 and decompose prevalence, mortality and DALYs by population age structure, population growth and epidemiologic changes.
Results: From 1992 to 2021, the worldwide prevalence of PAH remained steady, while mortality and DALYs associated with PAH declined. There were substantial disparities in the PAH burden and trends across sex, age and SDI regions. Population aging and growth were key factors driving the increase in PAH prevalence, while epidemiological changes affected DALYs differently across regions. Frontier analysis indicated that countries or regions with a higher SDI quintile tend to have greater improvement potential. Predictions suggested that from 2022 to 2046, global PAH prevalence, mortality, and DALYs were expected to decline, with persisting but decreasing gender differences.
Conclusions: The study provided a comprehensive global assessment of the PAH burden. Socioeconomic factors significantly influence PAH outcomes, highlighting the need for equitable access to healthcare access. Future projections indicate ongoing improvements in PAH management, underscoring the importance of continued research and policy development.
Keywords: Global Burden of Disease 2021 (GBD 2021); Pulmonary arterial hypertension (PAH); disability-adjusted life years (DALYs); mortality; prevalence.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-305/coif). The authors have no conflicts of interest to declare.
Figures



Similar articles
-
Global, regional, and national burden of maternal disorders, 1990-2021: a systematic analysis from the global burden of disease study 2021.BMC Public Health. 2025 Jul 29;25(1):2576. doi: 10.1186/s12889-025-23814-w. BMC Public Health. 2025. PMID: 40730990 Free PMC article.
-
The disproportionate burden of pulmonary arterial hypertension among the elderly: global, regional, and national trends from 1990 to 2021-findings from the 2021 global burden of disease study.Front Cardiovasc Med. 2025 Jul 8;12:1564785. doi: 10.3389/fcvm.2025.1564785. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40698002 Free PMC article.
-
Global pattern, trend and cross-country inequalities of inguinal, femoral, and abdominal hernia among individuals aged 60 and above from 1990 to 2021 and projections until 2040: a population-based study.Surg Endosc. 2025 Jul;39(7):4335-4344. doi: 10.1007/s00464-025-11810-5. Epub 2025 May 28. Surg Endosc. 2025. PMID: 40437076
-
National and subnational burden of brain and central nervous system cancers in China and global from 1990 to 2021: results from the global burden of disease study 2021.Arch Public Health. 2025 Jul 28;83(1):195. doi: 10.1186/s13690-025-01683-4. Arch Public Health. 2025. PMID: 40722045 Free PMC article.
-
The global burden of adverse effects of medical treatment: a 30-year socio-demographic and geographic analysis using GBD 2021 data.Front Big Data. 2025 Aug 1;8:1590551. doi: 10.3389/fdata.2025.1590551. eCollection 2025. Front Big Data. 2025. PMID: 40821361 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources