

The impact of extended lymphadenectomy on survival in esophageal adenocarcinoma with complete pathologic response: a retrospective study
- PMID: 40809202
- PMCID: PMC12340318
- DOI: 10.21037/jtd-2025-172
The impact of extended lymphadenectomy on survival in esophageal adenocarcinoma with complete pathologic response: a retrospective study
Abstract
Background: The impact of extended lymphadenectomy in esophageal adenocarcinoma (EAC) has been established in recent literature. The role of lymph node harvest in those achieving a complete pathologic response (CPR) is less clear. We aim to further investigate the impact of extended lymphadenectomy on survival in those patients with CPR.
Methods: The National Cancer Database (NCDB) was queried from 2006-2021 for patients with EAC without distant metastasis who received trimodal therapy. Groups of <10, 10-20, and >20 nodes harvested were established. Multivariable Cox regression and Kaplan-Meier survival analyses were conducted.
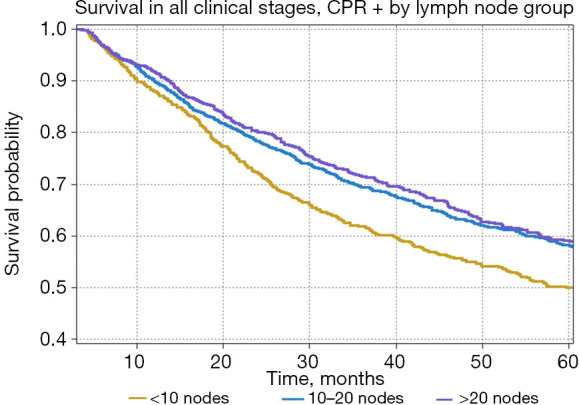
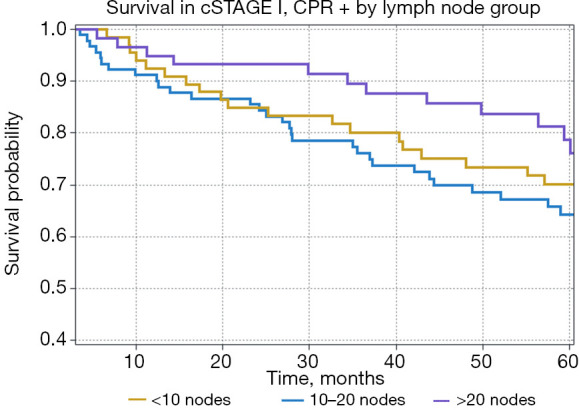
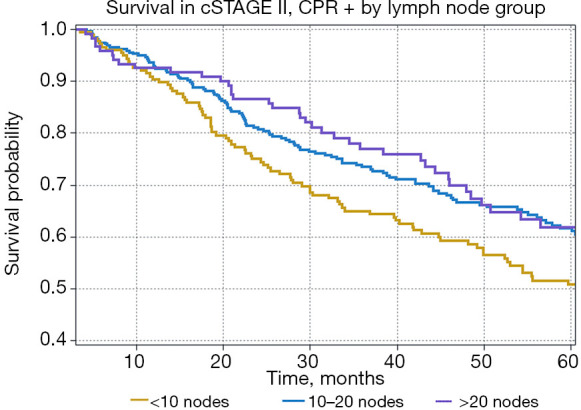
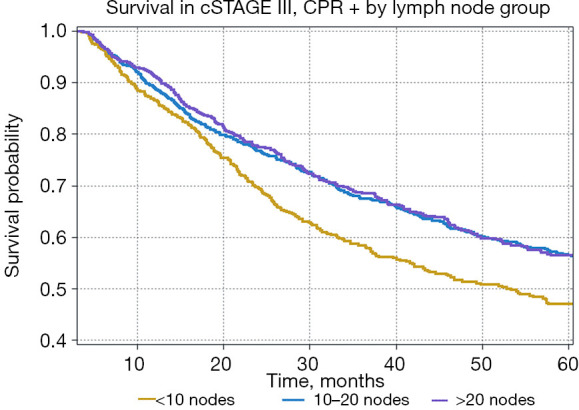
Results: Of 17,292 patients identified, 20.51% (n=3,547) had CPR. Multivariable analysis identified extended lymphadenectomy as an independent prognostic factor for survival in those with CPR [10-20 nodes, hazard ratio (HR) 0.847, P=0.03; >20 nodes, HR 0.768, P=0.01]. Median survival was longer in the 10-20 nodes (91.70 months) and >20 nodes (81.15 months) groups compared to the <10 nodes group (59.70 months, P=0.03), but similar between the 10-20 and >20 nodes groups (P=0.84). Analysis by clinical stage (cSTAGE) revealed no survival benefit with increasing nodal harvest in cSTAGE I (P=0.25) or cSTAGE II (P=0.12) disease. In those with cSTAGE III disease, increased nodal harvest served as an independent prognostic factor for survival (10-20 nodes HR 0.811, P=0.03; >20 nodes, HR 0.770, P=0.02). Median survival improved with 10-20 nodes (84.21 months) compared to <10 nodes (53.32 months, P=0.03) but not further with >20 nodes (74.64 months, P=0.74).
Conclusions: These results suggest that the benefit of lymphadenectomy in those with CPR may be stage dependent. In our cohort, only those with cSTAGE III disease saw a benefit from a greater than >10 nodes harvest and no groups derived additional benefit from more extended lymphadenectomy (>20 nodes).
Keywords: Esophageal cancer; complete pathologic response (CPR); lymph node metastases; lymphadenectomy.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-172/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Lymphadenectomy for the management of endometrial cancer.Cochrane Database Syst Rev. 2017 Oct 2;10(10):CD007585. doi: 10.1002/14651858.CD007585.pub4. Cochrane Database Syst Rev. 2017. PMID: 28968482 Free PMC article.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Lymphadenectomy for the management of endometrial cancer.Cochrane Database Syst Rev. 2015 Sep 21;2015(9):CD007585. doi: 10.1002/14651858.CD007585.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2017 Oct 02;10:CD007585. doi: 10.1002/14651858.CD007585.pub4. PMID: 26387863 Free PMC article. Updated.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
References
LinkOut - more resources
Full Text Sources