

Pregnancy in patients with pulmonary hypertension: a systematic review and meta-analysis with meta-regression
- PMID: 40809209
- PMCID: PMC12340376
- DOI: 10.21037/jtd-2025-430
Pregnancy in patients with pulmonary hypertension: a systematic review and meta-analysis with meta-regression
Abstract
Background: Pregnancy in patients with significant pulmonary hypertension (PH) is a contraindication due to high maternal and fetal mortality. However, recent data shows that an increasing number of women with PH are successfully carrying pregnancies to term, likely because of advancements in multidisciplinary care and treatment. This systematic review and meta-analysis aims to evaluate recent outcomes and identify risk factors associated with morbidity and mortality in this high-risk group.
Methods: An unrestricted search was conducted across MEDLINE, EMBASE, and Cochrane databases for studies on outcomes in pregnant patients with PH from inception until May 30, 2024. For one-group analyses, event rates and 95% confidence interval (CI) were calculated using a random-effects model. Meta-regression was performed with Comprehensive Meta-Analysis version 4, employing covariates in logistic regression models. For two-group comparisons, odd ratios (ORs) and 95% CIs were calculated using Review Manager version 5.4 utilizing a random-effects model.
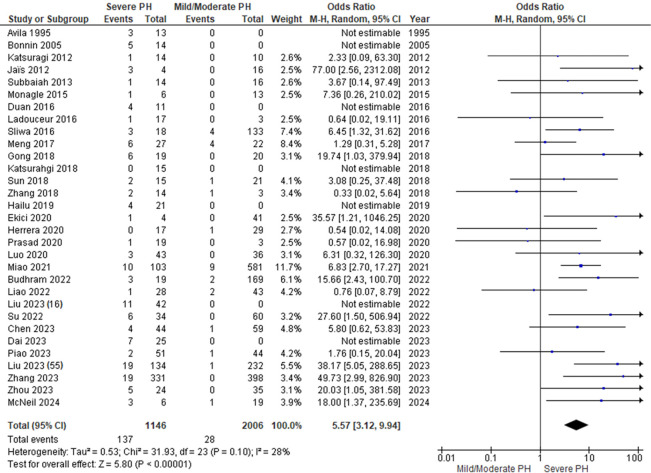
Results: Fifty-one studies involving 4,583 pregnant patients with PH were included. The maternal mortality rate was 7.6% (95% CI: 5.8-9.9%). Most deaths (93%) occurred in the postpartum period. Severe PH was associated with a significantly higher rate of maternal mortality compared to mild/moderate PH with OR 5.57 (95% CI: 3.12-9.94). Higher systolic pulmonary artery pressure (sPAP) was associated with a higher mortality rate with a regression coefficient of 0.96. Similarly, the presence of Eisenmenger syndrome (ES) was linked to a higher mortality rate with a regression coefficient of 1. Severe PH was also associated with higher rates of abortion (OR =3.64, 95% CI: 2.61-5.09), prematurity (OR =2.52, 95% CI: 1.66-3.81), and small gestational age (OR =3.96, 95% CI: 2.96-5.29) compared with mild/moderate PH.
Conclusions: Although the outcomes of pregnant patients with PH continue to improve, severe PH continues to be associated with a high mortality rate, abortion rate, prematurity, and small gestational age. Our findings support the existing consensus against pregnancy in severe PH and emphasize the need for thorough, individualized discussions about risks for patients with mild/moderate PH.
Keywords: Pulmonary hypertension (PH); maternal mortality; pregnancy; systolic pulmonary artery hypertension.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-430/coif). C.G.M. serves as an unpaid editorial board member of Journal of Thoracic Disease from February 2025 to January 2027. The other authors have no conflicts of interest to declare.
Figures

Similar articles
-
Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term.Cochrane Database Syst Rev. 2017 Jan 15;1(1):CD009273. doi: 10.1002/14651858.CD009273.pub2. Cochrane Database Syst Rev. 2017. PMID: 28106904 Free PMC article.
-
Incentives for increasing prenatal care use by women in order to improve maternal and neonatal outcomes.Cochrane Database Syst Rev. 2015 Dec 15;2015(12):CD009916. doi: 10.1002/14651858.CD009916.pub2. Cochrane Database Syst Rev. 2015. PMID: 26671418 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth.Cochrane Database Syst Rev. 2017 Mar 21;3(3):CD004454. doi: 10.1002/14651858.CD004454.pub3. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Dec 25;12:CD004454. doi: 10.1002/14651858.CD004454.pub4. PMID: 28321847 Free PMC article. Updated.
-
Immediate versus deferred delivery of the preterm baby with suspected fetal compromise for improving outcomes.Cochrane Database Syst Rev. 2016 Jul 12;7(7):CD008968. doi: 10.1002/14651858.CD008968.pub3. Cochrane Database Syst Rev. 2016. PMID: 27404120 Free PMC article.
References
LinkOut - more resources
Full Text Sources