

Lymph nodes metastatic burden as a prognosticator for advanced non-small cell lung cancer: a real-world study
- PMID: 40809212
- PMCID: PMC12340286
- DOI: 10.21037/jtd-2024-2201
Lymph nodes metastatic burden as a prognosticator for advanced non-small cell lung cancer: a real-world study
Abstract
Background: Current nodal classification inadequately predicts outcomes for advanced non-small cell lung cancer (NSCLC) patients. We investigated whether metastatic lymph node characteristics could improve prognostic accuracy.
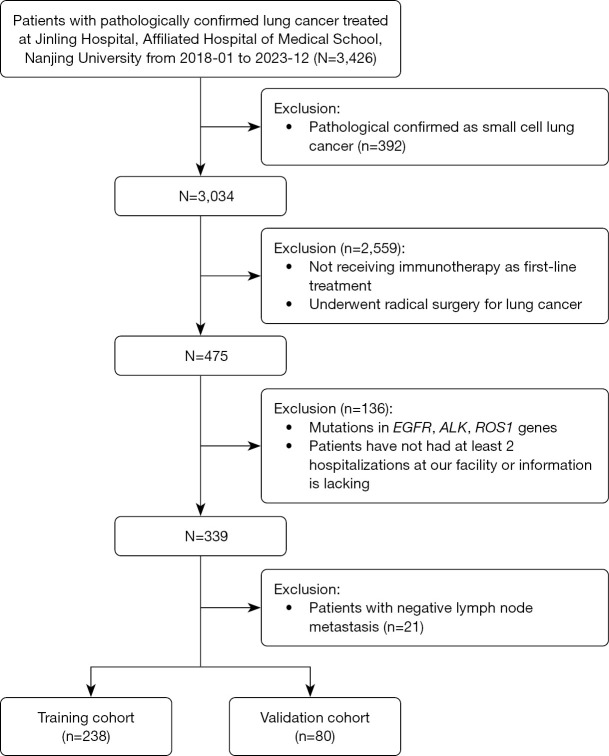
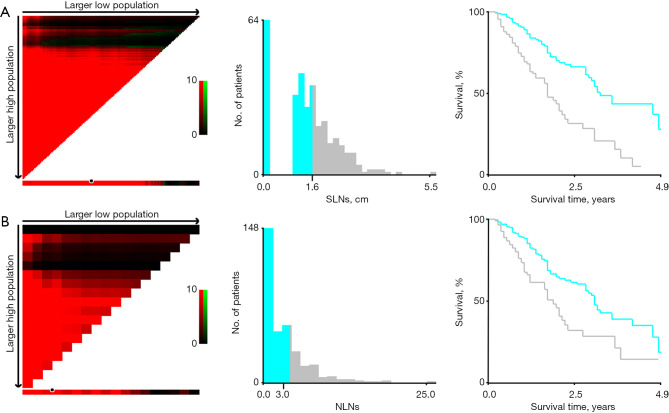
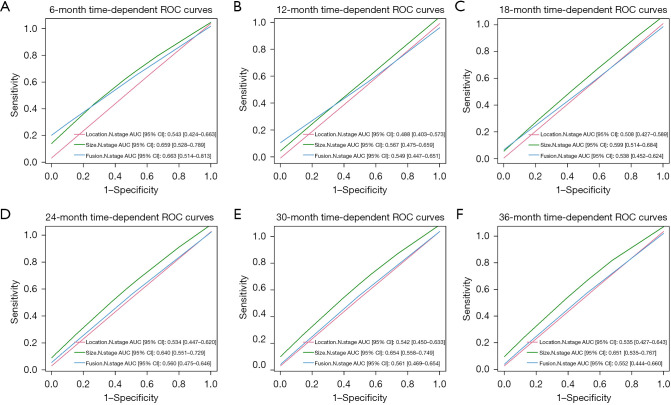
Methods: We retrospectively analyzed 339 patients with advanced NSCLC who received immunotherapy as first-line treatment. Lymph node imaging was performed using computed tomography (CT), and the X-tile software was employed to determine optimal cutoff values for lymph node size and number. Prognostic factors were assessed using Kaplan-Meier survival curves and multivariate Cox regression analysis. The predictive accuracy of various N-staging was evaluated through time-dependent receiver operating characteristic (ROC) curves.
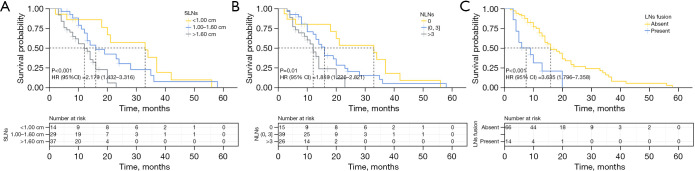
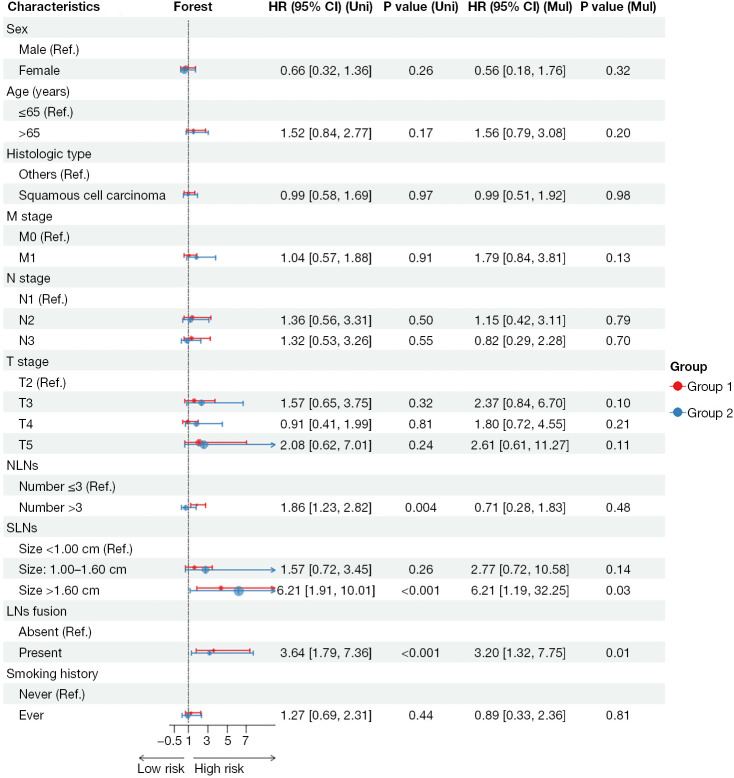
Results: The optimal cutoff values for lymph node size and number were 1.60 cm and 3, respectively. Kaplan-Meier analysis indicated that size, number, and fusion of metastatic lymph nodes were associated with worse overall survival (OS) in advanced NSCLC patients {hazard ratio (HR) [95% confidence interval (CI)]: 2.179 (1.432-3.316), 1.859 (1.226-2.821), and 3.635 (1.796-7.358)}. Multivariate Cox regression analysis identified lymph node size [HR (95% CI): 6.21 (1.19-32.25)] and fusion [HR (95% CI): 3.20 (1.32-7.75)] as independent prognostic factors for OS. Incorporating lymph node size into the conventional N-staging system improved prognostic accuracy, with a 3-year area under the curve (AUC) of 0.651 (95% CI: 0.535-0.767).
Conclusions: Lymph node size serves as a valuable indicator of tumor invasion and can enhance the existing N-staging system for more accurate prognosis prediction for more accurate prognosis prediction in advanced NSCLC.
Keywords: Lymph node staging; immunotherapy; metastatic burden; non-small cell lung cancer (NSCLC); prognosis.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2024-2201/coif). All authors report that this study was supported by Jinling Hospital Management Project grants 22LCYY-XH2 (H.L.). The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
PET-CT for assessing mediastinal lymph node involvement in patients with suspected resectable non-small cell lung cancer.Cochrane Database Syst Rev. 2014 Nov 13;2014(11):CD009519. doi: 10.1002/14651858.CD009519.pub2. Cochrane Database Syst Rev. 2014. PMID: 25393718 Free PMC article.
-
Lymph node ratio emerges as a pivotal prognostic determinant for cancer-specific survival amidst individuals diagnosed with stage N1 and N2 non-small cell lung carcinoma: A population-based retrospective cohort study.Medicine (Baltimore). 2025 Apr 18;104(16):e42202. doi: 10.1097/MD.0000000000042202. Medicine (Baltimore). 2025. PMID: 40258731 Free PMC article.
-
Sublobar resection is non-inferior to lobectomy in octogenarians and older with stage Ia non‑small cell lung cancer.Transl Cancer Res. 2025 May 30;14(5):2966-2980. doi: 10.21037/tcr-2024-2575. Epub 2025 May 14. Transl Cancer Res. 2025. PMID: 40530121 Free PMC article.
-
Rationality of FIGO 2018 IIIC cervical cancer according to local tumor and pelvic lymph node metastatic extent-a cohort study.BMC Womens Health. 2025 Jul 4;25(1):308. doi: 10.1186/s12905-025-03846-5. BMC Womens Health. 2025. PMID: 40616036 Free PMC article.
-
Diagnostic accuracy of endoscopic ultrasonography (EUS) for the preoperative locoregional staging of primary gastric cancer.Cochrane Database Syst Rev. 2015 Feb 6;2015(2):CD009944. doi: 10.1002/14651858.CD009944.pub2. Cochrane Database Syst Rev. 2015. PMID: 25914908 Free PMC article.
References
LinkOut - more resources
Full Text Sources