

Tailored single-lung ventilation approaches and postoperative pulmonary outcomes in thoracic surgery
- PMID: 40809239
- PMCID: PMC12340303
- DOI: 10.21037/jtd-2025-314
Tailored single-lung ventilation approaches and postoperative pulmonary outcomes in thoracic surgery
Abstract
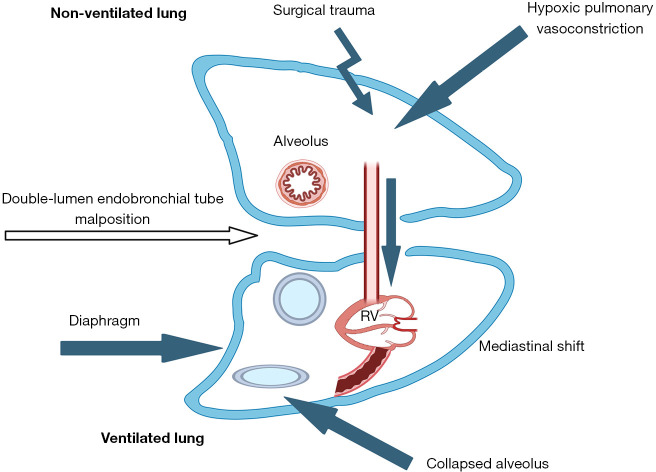
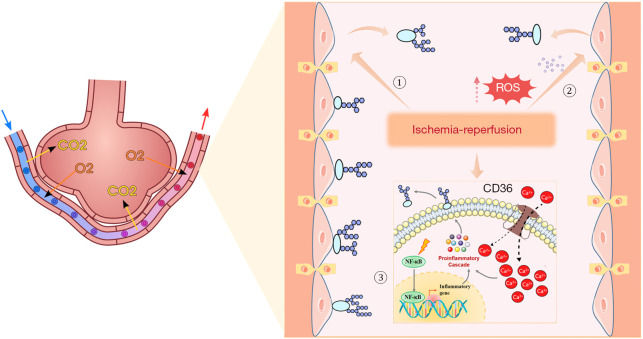
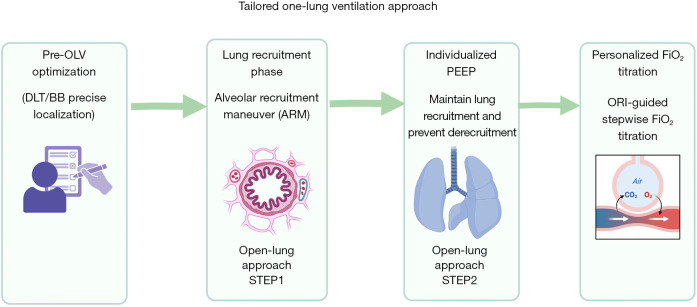
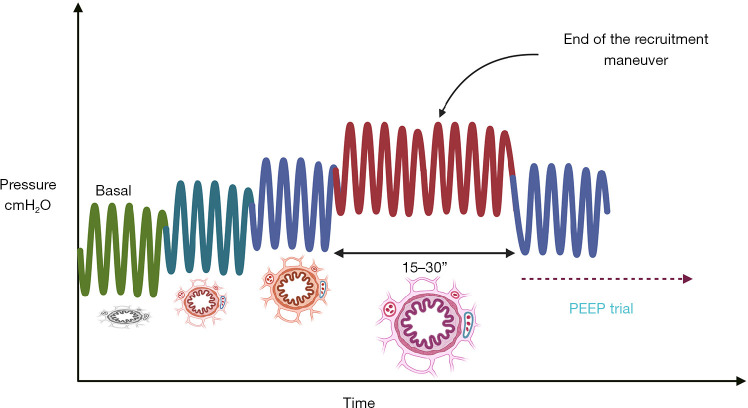
Traditional lung-protective ventilation [low tidal volume (VT) with fixed positive end-expiratory pressure (PEEP)] reduces intraoperative lung injury but exhibits limited efficacy in preventing postoperative pulmonary complications (PPCs) following thoracic surgery requiring one-lung ventilation (OLV). This review systematically examines the multifactorial mechanisms of OLV-associated lung injury, encompassing hypoxemia [device malposition, atelectasis, ventilation/perfusion (V/Q) mismatch, impaired hypoxic pulmonary vasoconstriction (HPV)], oxidative stress, ischemia-reperfusion injury (IRI) (glycocalyx degradation, mechanical stress, inflammation), and ventilator-induced trauma (volutrauma, biotrauma). To address these limitations, we propose an open-lung protective ventilation strategy integrating alveolar recruitment maneuvers (RMs) with individualized PEEP (iPEEP) titration based on optimal respiratory compliance. Furthermore, we innovatively introduce oxygen reserve index (ORI)-guided titration of fraction of inspired oxygen (FiO2), enabling dynamic determination of the minimum effective FiO2 to mitigate hyperoxia-related toxicity. This synergistic "RM-iPEEP-FiO2 triad" facilitates personalized intraoperative respiratory management by stabilizing alveoli, optimizing V/Q matching, and minimizing oxidative stress, thereby significantly reducing PPCs risk compared to conventional fixed-parameter approaches. Current limitations include insufficient multicenter validation, technical dependency on advanced monitoring/ventilators, and lack of subgroup analyses for high-risk populations. Future research should prioritize multicenter randomized controlled trials to establish universal thresholds for tailored parameters. Integration of artificial intelligence (AI) for real-time respiratory mechanics analysis and multimodal imaging is essential to refine precision thresholds. Ultimately, this strategy aims to establish an evidence-based, precision perioperative ventilation framework that optimizes clinical outcomes in thoracic surgical patients by overcoming the constraints of standardized ventilation protocols.
Keywords: One-lung ventilation (OLV); lung injury; mechanical ventilation; postoperative pulmonary complications (PPCs); tailored lung protective ventilation strategies.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-2025-314/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Ventilator Management(Archived).2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Mar 27. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28846232 Free Books & Documents.
-
Effects of Individualized Positive End-Expiratory Pressure on Patients Undergoing One-Lung Ventilation During Thoracic Surgery: A Systematic Review and Meta-Analysis.J Cardiothorac Vasc Anesth. 2025 Jul 11:S1053-0770(25)00483-5. doi: 10.1053/j.jvca.2025.06.019. Online ahead of print. J Cardiothorac Vasc Anesth. 2025. PMID: 40783324 Review.
-
Optimized ventilation strategy for surgery on patients with obesity from the perspective of lung protection: A network meta-analysis.Front Immunol. 2022 Oct 18;13:1032783. doi: 10.3389/fimmu.2022.1032783. eCollection 2022. Front Immunol. 2022. PMID: 36330511 Free PMC article.
-
An optimal protective ventilation strategy in lung resection surgery: a prospective, single-center, three-arm randomized controlled trial.Updates Surg. 2025 Jun;77(3):925-935. doi: 10.1007/s13304-025-02091-7. Epub 2025 Jan 21. Updates Surg. 2025. PMID: 39838183 Free PMC article. Clinical Trial.
-
Intraoperative ventilation strategies to prevent postoperative pulmonary complications: Systematic review, meta-analysis, and trial sequential analysis.Best Pract Res Clin Anaesthesiol. 2015 Sep;29(3):331-40. doi: 10.1016/j.bpa.2015.09.002. Epub 2015 Sep 18. Best Pract Res Clin Anaesthesiol. 2015. PMID: 26643098
References
-
- Smith S, Arthur ME. Lung Isolation Anesthesia. 2025. - PubMed
Publication types
LinkOut - more resources
Full Text Sources